Marketing to Doctors: The Data-Driven Playbook for 2026
Half the advice online about marketing to doctors is actually about marketing for doctors - helping practices get more patients. That's not what you're here for. You're trying to reach physicians as a B2B audience: selling them software, devices, therapeutics, or services. It's a $24.77B digital ad market growing 13%+ year over year, but the playbook looks nothing like standard B2B.
The biggest mistake we see teams make is treating physicians like any other persona. They're not. Doctors are time-starved, skeptical of sales pitches, and trained to evaluate evidence before making decisions. The channels that work, the messaging that converts, and the compliance rules that govern every interaction are all specific to this audience. Get any of those wrong and you're not just wasting budget - you're burning trust with a community that talks.
The Short Version
Physicians prefer email and endemic medical platforms for staying current. Point-of-care is the fastest-growing channel nobody's talking about - up 171% since 2019. Pick three channels, execute them flawlessly, and verify every contact before you send a single message. That last part trips up more teams than you'd think.
Which Channels Actually Work?
A Mediately survey of ~1,680 physicians across 9 countries found that email and phone alerts were the preferred way to receive updates on new treatments, followed by in-person rep meetings, then webinars and virtual events. That tracks with everything else we see in the data.
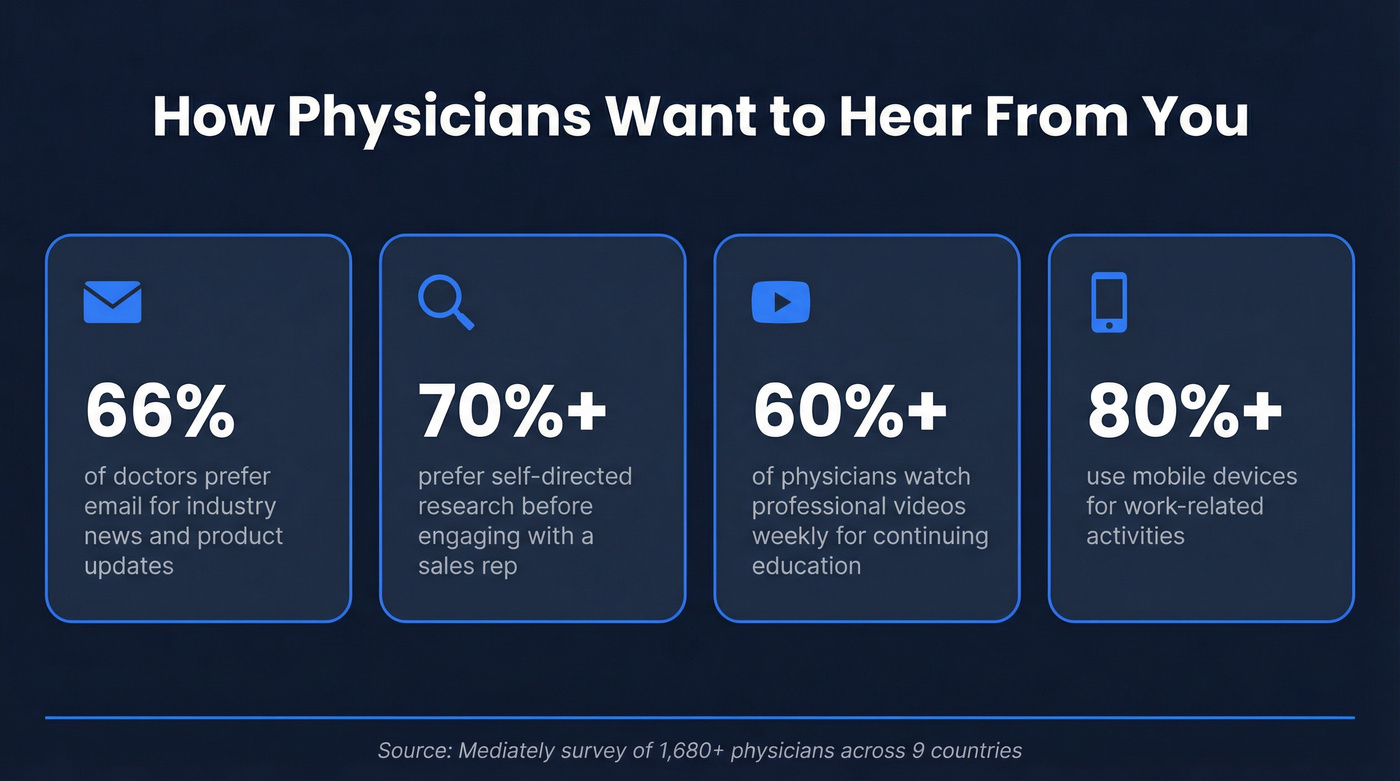
66% of doctors prefer email for industry news, product updates, and research. Over 70% prefer self-directed research before engaging with a sales rep. Those two stats alone should reshape how you sequence your outreach.
On the content side, 60%+ of physicians watch professional videos weekly for continuing education, and 80%+ use mobile devices for work-related activities. Your subject lines, landing pages, and content all need to be mobile-first - not mobile-friendly as an afterthought.
Here's the thing: doctors want to consume information on their own terms, in formats they control. Email lets them do that. Endemic platforms like Doximity and Medscape meet them where they're already spending time. Reps and events still matter, but they're closers, not openers.
The Channel Playbook
Email Marketing
Email is a top physician-preferred channel, and it's also the cheapest to execute - if your list is clean. The tactical details matter more here than in standard B2B email.
The optimal body copy range is 50-125 words, with 75-100 words being the sweet spot where response rates are strongest for physician audiences. Subject lines should run ~29 characters for mobile and ~35 for desktop, which means 3-4 words max. Preheaders need to be 35-53 characters on mobile. Physicians are scanning on their phones between patients. You need to be instantly clear.
For sustained nurture, twice a month works. For a 30-day product launch push, weekly is acceptable. Go beyond that and you'll pay for it in engagement and list fatigue. In our experience, the 75-word sweet spot holds across specialties - cardiologists and dermatologists alike will ignore a 300-word email.
Endemic Platforms
Endemic platforms like Doximity, Medscape, and Sermo let you reach physicians inside the professional tools they already use daily. These aren't cheap, but they deliver qualified impressions you can't get on the open web.
| Platform | Est. Reach | Est. CPM | Best For |
|---|---|---|---|
| Doximity | Large US physician audience | $40-80 | Targeted display, messaging |
| Medscape/WebMD Pro | Broad HCP base | $30-60 | Sponsored content, awareness |
| Sermo | Large physician community | Custom ($10K-30K/campaign) | Peer engagement, surveys |
Minimum campaign spends typically run $25K-50K+ on Doximity. Medscape packages start around $15K. Secondary endemic options worth exploring include UpToDate, Healio, and Epocrates - all places physicians go for clinical decision support, which means high-intent eyeballs.
Full Channel Comparison
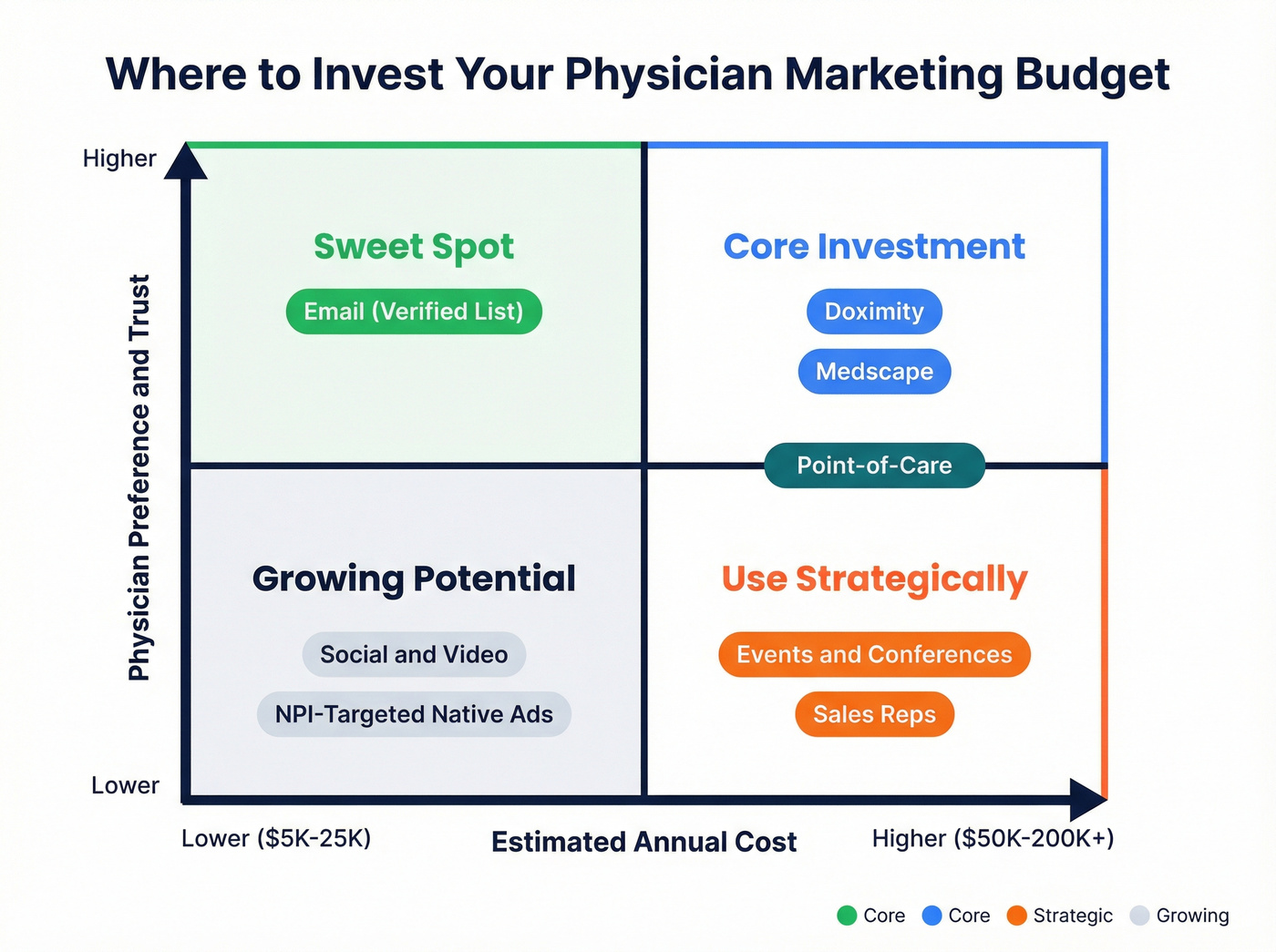
Here's how every major channel stacks up. If you only have budget for three, start with the ones marked "Core."
| Channel | Est. Annual Cost | Physician Preference | Best For | Priority |
|---|---|---|---|---|
| Email (verified list) | $5K-25K | Highest (66% prefer) | Nurture, product launches | Core |
| Doximity | $25K-75K | High (endemic trust) | Targeted awareness, messaging | Core |
| Medscape | $15K-60K | High (endemic trust) | Sponsored content, broad reach | Core |
| Point-of-Care | $20K-80K | Medium-High (clinical context) | Decision-point influence | High |
| NPI-Targeted Native (Tap Native) | $15K-50K | Medium | Attribution-rich display | Medium |
| Events & Conferences | $25K-200K+ | Medium (73.5% marketer usage) | Relationship building, closing | Medium |
| Social & Video | $10K-50K | Growing (60%+ watch weekly) | Education, thought leadership | Growing |
Native & Programmatic HCP Ads
Standard display banners don't work for physicians. Banner blindness is real, and it's worse in healthcare because doctors are trained to filter noise.
Tap Native is the clearest example of NPI-based 1:1 targeting - 7.2 million NPIs across 360+ specialties, with ads only served when the platform knows exactly who's viewing the page. CPCs start at $5+ and climb as targeting narrows. NP and PA clicks run cheaper than MD clicks, which matters for budget planning.
The real value is in the reporting. Tap Native provides PLD (provider-level data) reports for every click - full name, NPI, specialty, and timestamp. That's attribution you can't get from programmatic display.
Point-of-Care Marketing
This is the channel most B2B healthcare marketers are underweighting. Point-of-care marketing hit $803M in 2023, up 171% since 2019 - roughly 22% annual growth. And that's just from 17 POCMA members reporting; the real market is likely north of $1B.
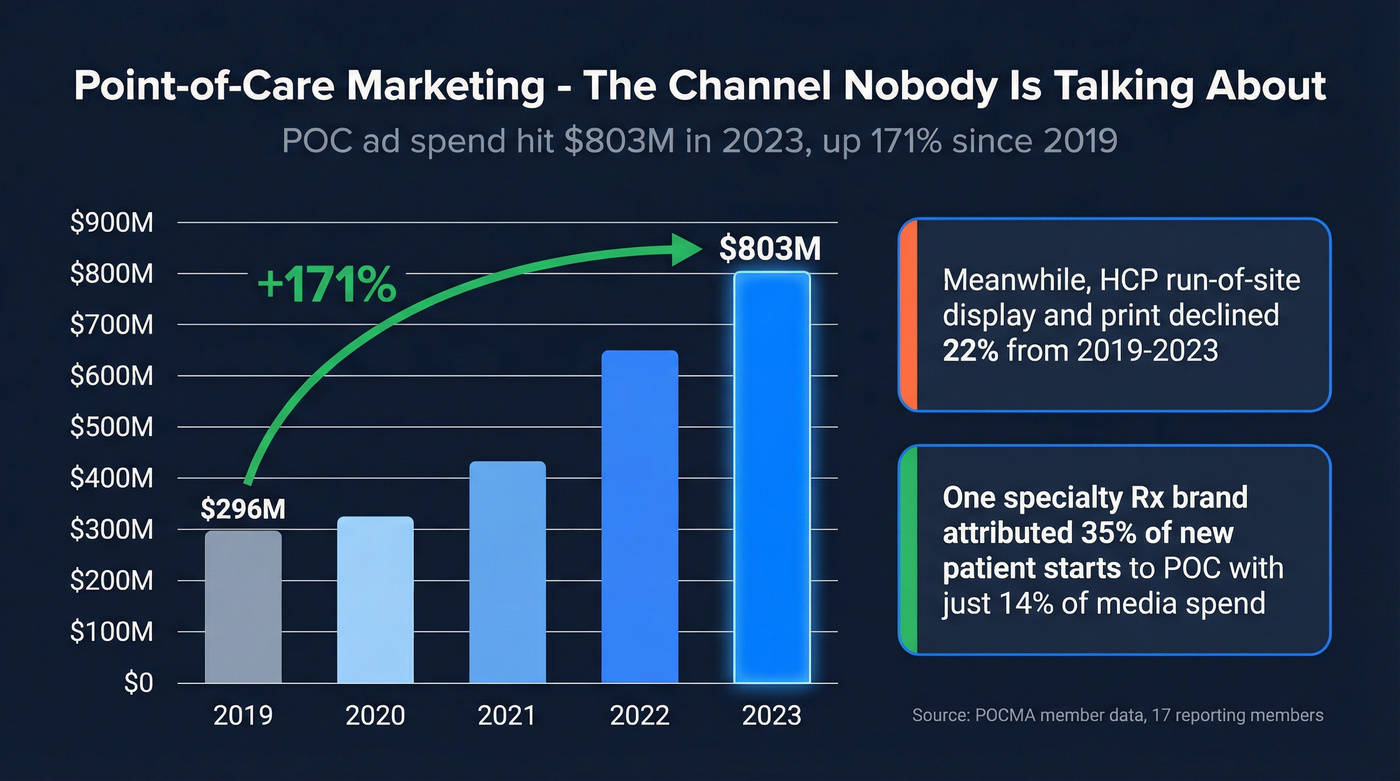
The formats include waiting room screens, exam room displays, and EHR integrations. One specialty Rx brand attributed 35% of new patient starts to POC with just 14% of media spend. We've seen POC consistently outperform run-of-site display in every campaign we've analyzed - the clinical context makes the difference. CPMs run $20-60, competitive with endemic platforms but with the added advantage of reaching physicians at the moment of clinical decision-making. Meanwhile, HCP run-of-site digital display and print declined 22% from 2019-2023. The money is moving for a reason.
Events, Conferences & Sales Reps
Events are back. Professional meetings and conferences hit 73.5% marketer usage in 2024, up from 59%. Sales reps as a channel rose to 60.2% from 56%. Booth sponsorships typically range from $5K to $50K+ depending on the conference tier.
But 70%+ of HCPs do their own research before they'll engage with a rep. Reps aren't discovery tools anymore - they're conversion tools. The best-performing teams use email and endemic content to warm physicians up, then deploy reps to close. If your reps are still cold-calling into physician offices, you're burning money and goodwill.
Social Media & Video
76.1% of healthcare marketers plan to increase social media spend, and the shift is toward "pull" content rather than push. 60%+ of HCPs watch professional videos weekly, which makes video and webinar formats the highest-leverage social play.
Doximity functions as the professional network for physicians - think of it as the endemic social channel. Beyond that, YouTube medical education content, branded webinars, and podcast sponsorships are all gaining traction. Digital Opinion Leaders are emerging as the physician equivalent of B2B influencers, with conversations moving to threads, podcasts, and specialized virtual communities. DOL programs are still early, but the trajectory is clear - physician audiences trust peer voices more than brand voices.
Your physician email campaigns are only as good as your list. Prospeo delivers 98% email accuracy with 7-day data refresh - so you're never emailing a doctor who left their practice six weeks ago. Filter by job title, specialty, and company to build targeted HCP lists in minutes.
Stop burning physician trust with bounced emails. Start with verified data.
Sunshine Act Compliance
If you're selling to physicians in the US, the Sunshine Act isn't optional knowledge - it's operational infrastructure. Every transfer of value to a physician or teaching hospital gets reported to CMS through Open Payments.
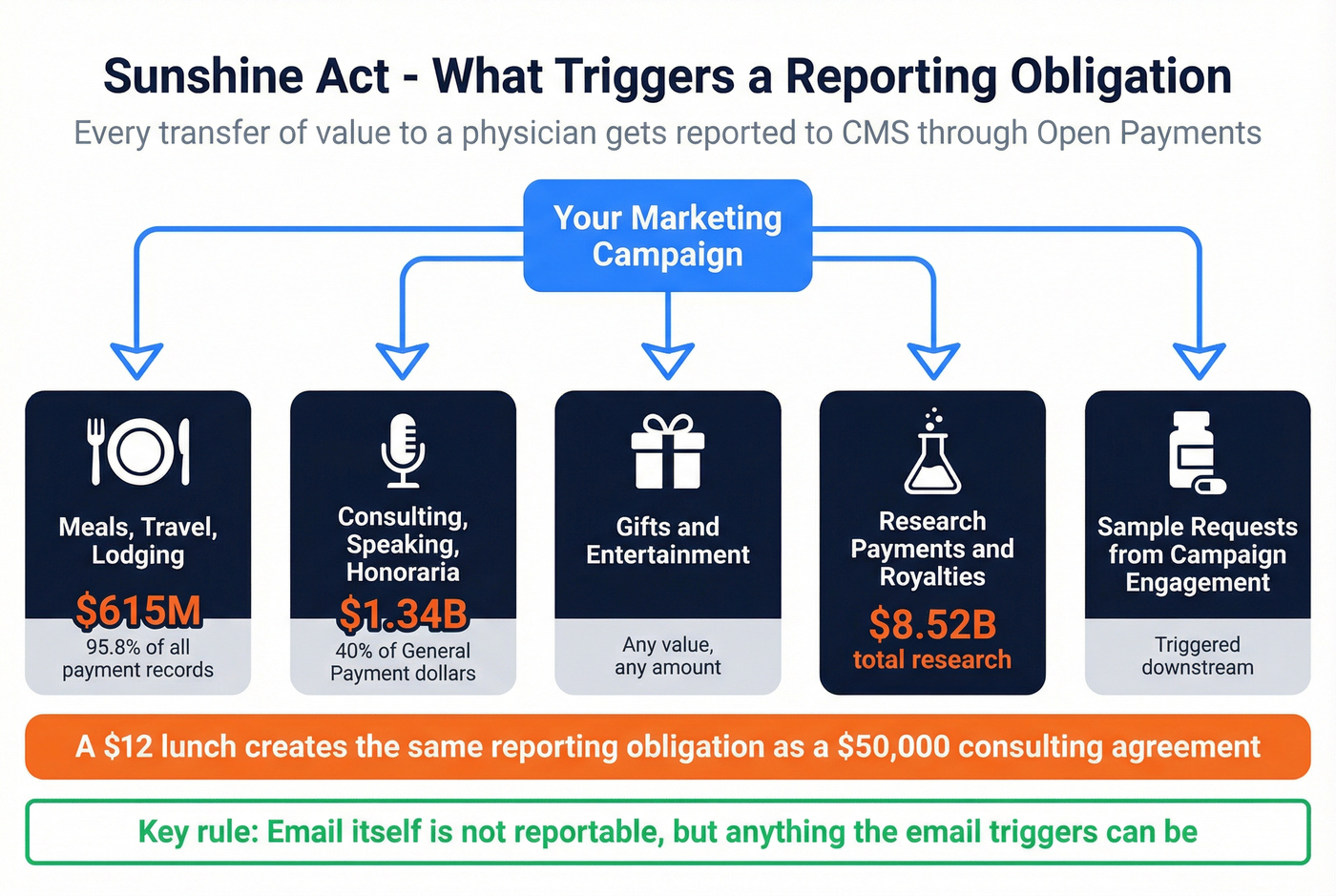
The 2024 numbers tell the story: 16.16 million records totaling $13.18B+. Of that, $8.52B was research-related. The General Payments breakdown is where it gets operationally painful.
Consulting, honoraria, and speaking fees account for $1.34B - 40% of General Payments dollars across 500K+ records. That's your KOL and speaker programs. Meals, travel, and lodging are $615M but represent 95.8% of General Payments records. Read that again - a $12 lunch creates the same reporting obligation as a $50,000 consulting agreement. The compliance ops burden is driven by volume, not dollar amount.
Reporting triggers - check every one before scaling:
- Any meal, gift, or travel provided to a physician
- Consulting or speaking fees, including advisory boards
- Grants and charitable contributions ($125.9M across fewer than 10K transactions in 2024)
- Research payments and royalties
- Sample requests triggered by campaign engagement
The PhRMA Code provides voluntary guidelines, but most large manufacturers treat them as mandatory. If you're running email campaigns that lead to dinner events, speaker programs, or sample requests, every downstream transfer of value needs tracking. Email itself isn't reportable - but anything the email triggers can be.
Let's be honest: most compliance failures at scale aren't about intent. They're about ops teams that can't track 50,000 meal transactions across 200 reps. Build the tracking infrastructure before you scale the programs.
Building a Verified Physician Contact List
You know which channels work. The operational gap is getting clean physician data to execute against them. NPI databases exist, but they're built for claims processing, not outreach - no verified emails, no direct dials, no segmentation by buying behavior. Whether you're focused on doctors in private practice or targeting hospitals with complex buying committees, the data challenge is the same.
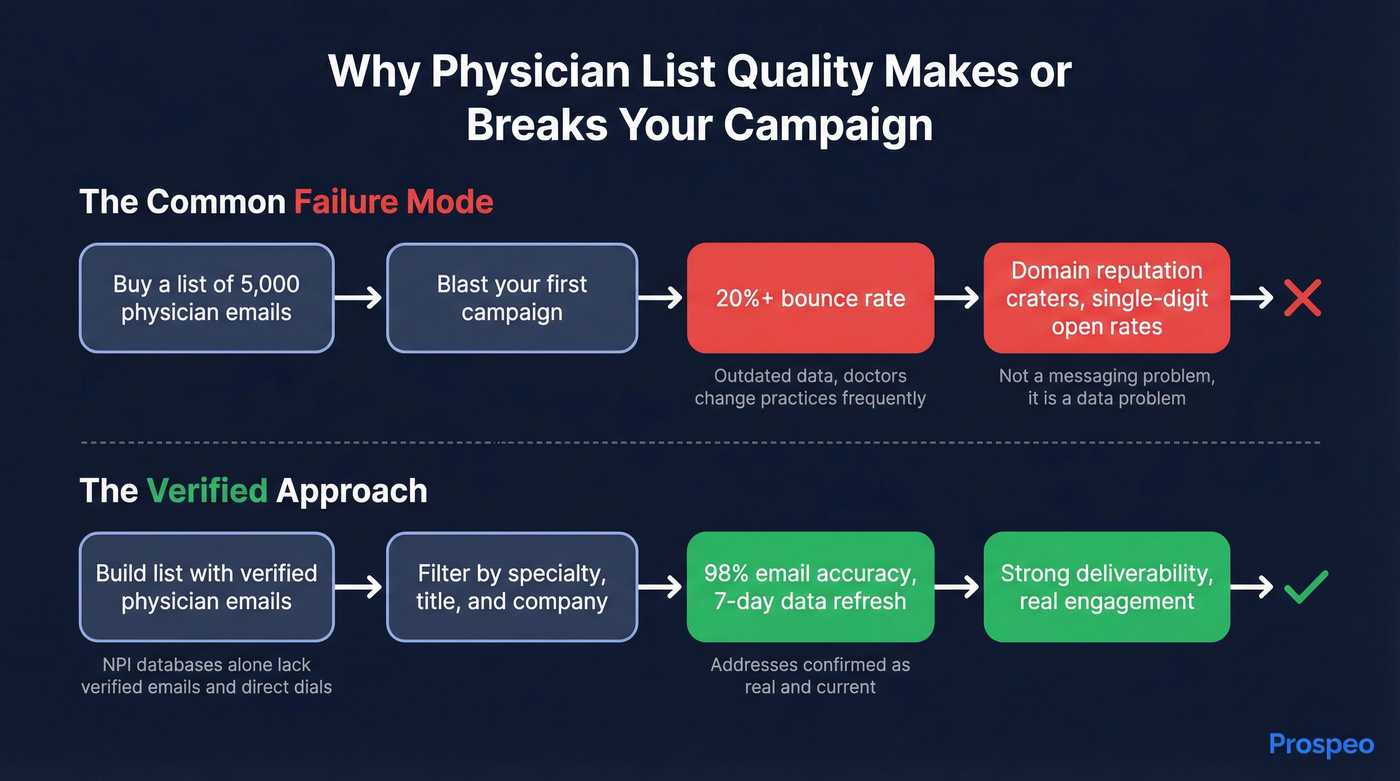
The failure mode is predictable and frustrating: you buy a list of 5,000 physician emails, blast your first campaign, hit a 20%+ bounce rate, and watch your domain reputation crater. Your single-digit open rate isn't a messaging problem - it's a data problem. Email is a top physician-preferred channel, but it only works if the addresses are real.
Prospeo solves this at the data layer. The platform covers 300M+ professional profiles with 98% email accuracy, verified through a proprietary 5-step process that catches spam traps, honeypots, and catch-all domains before they damage your sender reputation. You can filter by job title, company size, and industry using 30+ search criteria to build targeted physician lists, and every record refreshes on a 7-day cycle - which matters in healthcare where physicians change affiliations frequently. Layer Bombora intent data across 15,000 topics to identify organizations actively evaluating solutions in your category. Pricing runs ~$0.01 per email with a free tier of 75 verified emails per month, fully self-serve, no contracts.
If you're worried about bounces and sender reputation, run an email deliverability checklist before you scale volume.
KOL & Speaker Programs
Key Opinion Leader programs remain one of the highest-impact channels for reaching physicians, and they're also one of the most compliance-intensive. The $1.34B in reported consulting and speaking payments tells you how much the industry invests here.
The KOL lifecycle runs from identification and contracting through segmentation, insights gathering, analysis, and post-engagement follow-up. What's changing is the definition of "KOL" itself - it's expanding beyond physicians to include patients, caregivers, and payers as stakeholders who shape clinical decisions.
Digital Opinion Leaders are the emerging frontier. DOL conversations happen on threads, podcasts, and virtual communities rather than conference stages. AI is accelerating KOL identification by scanning publication records, citation networks, and social engagement to surface rising voices. But it introduces risks around inaccuracy and credibility erosion - an AI-recommended KOL who turns out to have thin credentials damages your brand with the physician audience faster than almost anything else. Build your KOL programs with Sunshine Act reporting baked in from day one, not bolted on after.
Budget Benchmarks
The MM+M/Swoop survey pegged the mean healthcare marketing budget at $7.2M in 2024 - the lowest in five years. Budgets are tighter, which makes channel selection more important than ever.
You don't need all seven channels. You need three, executed flawlessly. For teams under $500K in total budget, start with email, one endemic platform, and point-of-care. Over $1M, add NPI-targeted native, events, and KOL programs.
If your average contract value is under $25K, skip endemic platform spend entirely. A verified email list, a tight 5-touch sequence, and one well-chosen conference will outperform a $50K Doximity campaign nine times out of ten. The endemic platforms shine when you need broad specialty-level awareness - not when you're selling to 200 target accounts.
Stop spending on HCP run-of-site display. It declined 22% from 2019-2023 because it doesn't work. Redirect those dollars to POC and verified email - channels where you can actually measure physician engagement at the individual level. And none of these email tactics matter if your list is dirty. Verify every address before sending. At $0.01 per verified email through Prospeo, it's a rounding error in your budget that prevents the most expensive mistake in physician outreach.
If you're building a repeatable outbound motion, use a documented outbound email campaign process and a clear sales cadence so reps and marketing stay aligned.
Reps need direct dials to reach doctors between patients. Prospeo has 125M+ verified mobile numbers with a 30% pickup rate - that's 3x the industry average. At $0.10 per number, you'll spend less on contacts than a single Doximity impression.
Give your reps verified physician mobiles that actually get answered.
FAQ
What's the most effective channel for reaching physicians?
Email - 66% of physicians prefer it for industry updates, and it delivers the highest ROI when your list is verified and messages stay under 100 words. Pair it with an endemic platform like Doximity or Medscape for awareness, and you've covered the two highest-preference channels.
How do you market to doctors in a way that converts?
Lead with value-driven email and endemic content that lets physicians self-educate, then deploy reps and events to close. Over 70% of HCPs research independently before engaging a sales rep - cold outreach without a warm-up sequence wastes budget and erodes credibility.
How much does it cost to advertise on Doximity or Medscape?
Expect $40-80 CPM for targeted physician impressions on Doximity, with minimum campaign spends of $25K-50K+. Medscape packages start around $15K-30K for sponsored content and display. Both platforms price based on specialty targeting and audience size.
Do I need to worry about the Sunshine Act for email campaigns?
Email itself isn't a reportable event under Open Payments. But any transfer of value the campaign triggers - meals, honoraria, gifts, travel - must be reported to CMS. In 2024, CMS logged $13.18B across 16.16M+ records. Even a $12 lunch counts.
How do I build a physician email list without bad data?
Use a verified B2B database - filter by job title, company, and industry, then verify every address in real time before sending. At 98% accuracy and $0.01 per verified email, this approach protects your domain reputation while keeping costs minimal.