How to Automate Sales Outreach in Healthcare Without Breaking Compliance
Picture this: you're a Series A healthtech startup with two SDRs, a TAM of maybe 4,000 hospital systems, and a compliance memo from legal that basically says "don't email anyone until we figure out HIPAA." Meanwhile, your board wants pipeline. That tension - between compliance paralysis and growth pressure - is where most healthcare teams trying to build automated outreach get stuck.
Here's the thing: the compliance barrier is real, but it's also smaller than most teams think. The actual rules are clear. The problem is that nobody explains them in plain English alongside a workable playbook. That's what this article does.
What You Need (Quick Version)
Healthcare outreach automation requires a compliance-first stack: a HIPAA-aware CRM, a verified data layer, and a sequencing tool with real deliverability infrastructure. Start with data quality - healthcare lists decay faster than any other vertical, and bounced emails to a TAM of a few thousand physicians will torch your sender domain.
Why Healthcare Outreach Automation Is Different
Generic sales automation tools aren't built for healthcare. The buying process alone should tell you that - and the same lesson applies if you sell to multiple verticals. What works for outbound SaaS or cold outreach in real estate will fail spectacularly in a clinical environment.

Healthcare buying committees average 22 decision-makers. Not 22 people who need to be informed - 22 people with veto power or sign-off authority. The average deal takes 14.7 months from initial contact to signature. Deals move sideways, stall for security reviews, restart after a vendor risk assessment, then stall again when procurement cycles kick in. You can't brute-force this with a 5-email drip and a calendar link.
Generic mass messaging is the fastest way to burn your domain and your reputation with a finite buyer pool. The messaging that converts centers on patient outcomes, regulatory compliance, ROI, and clinical validation - not urgency, not FOMO, not "limited spots available."
HIPAA Compliance for Outreach Automation
Most healthcare sales teams overcorrect on HIPAA. Cold outreach using business contact information - name, work email, title - isn't a HIPAA violation. PHI is the trigger. Keep patient data, clinical records, and insurance details out of your sequences entirely, and you're operating in a PHI-free workflow.
We've seen teams sit paralyzed for months over compliance concerns that don't actually apply to their outreach. The compliance paralysis is worse than the actual compliance requirements.
That said, many organizations apply HIPAA email rules to all email because separating PHI from non-PHI traffic is operationally messy. If your org takes that approach, your email infrastructure needs:
- A signed Business Associate Agreement (BAA) - non-negotiable
- Encryption in transit (TLS) and at rest
- Role-based access controls and audit logging
- Breach notification within 60 days
- "Minimum necessary" data principle (§164.502(b))
The penalty range for violations runs $100-$50,000 per violation, with a $1.5M/year cap for the same provision. That's enough to kill a startup.
| Provider | BAA Available? | Price |
|---|---|---|
| Amazon SES | Yes (AWS BAA) | $0.10/1K emails |
| Mailgun | Enterprise plans | Custom pricing |
| SendGrid (Twilio) | Pro+/Enterprise | Custom pricing |
For most healthtech teams, Amazon SES with CloudTrail audit logging is the cost-effective starting point.
TCPA 2025 Rules - What Changed for Outbound
The FCC's updated opt-out rules went into effect April 11, 2025, and they fundamentally changed how automated outreach works. If you don't have a solid opt-out management process, these rules will catch you off guard.
If you're also running SMS, treat this like regulated outbound from day one and align it with your broader cold texting policy.
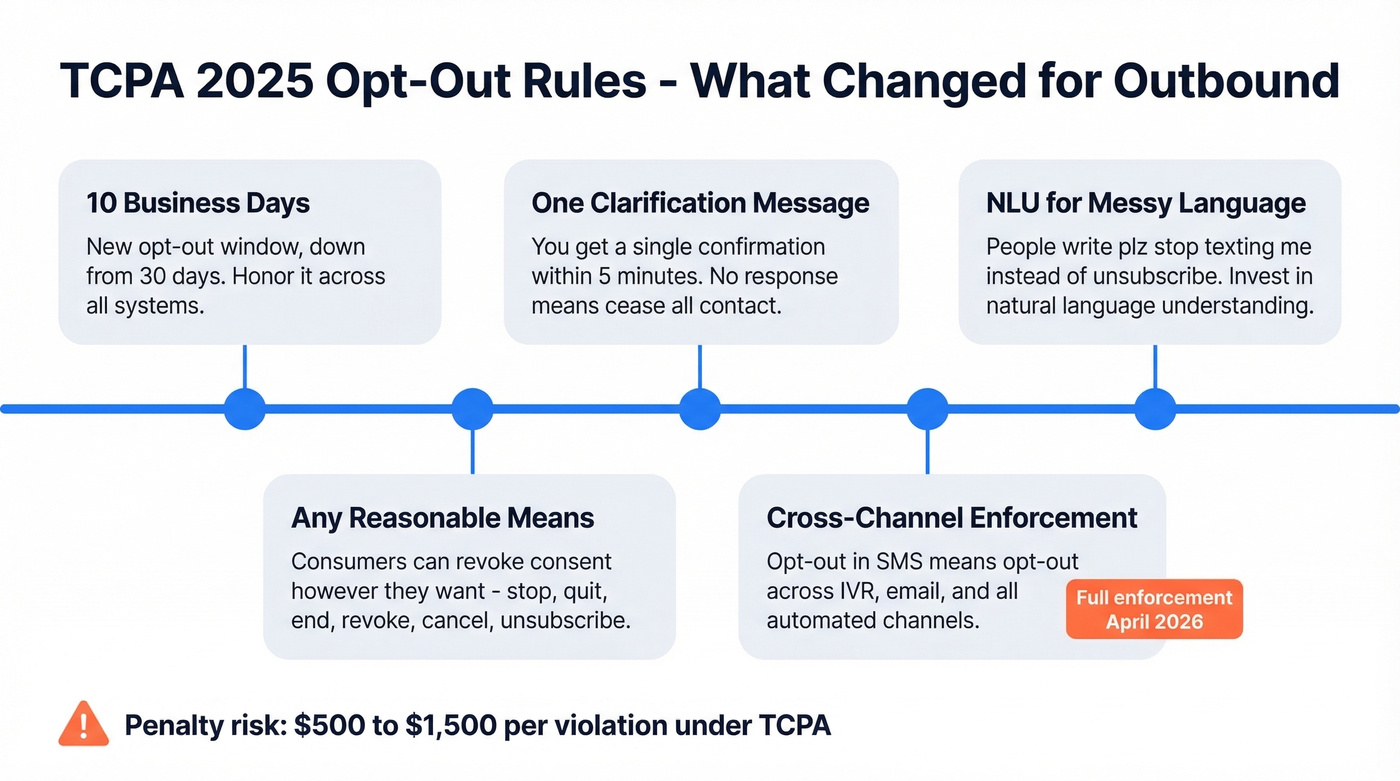
10-business-day opt-out window. Down from 30 days. When someone says stop, you have 10 business days to honor it across your systems.
"Any reasonable means" language. Consumers can revoke consent however they want. The FCC lists per se reasonable words: "stop," "quit," "end," "revoke," "opt out," "cancel," "unsubscribe."
One clarification message within five minutes. You get a single shot to confirm the opt-out request. No response? Cease all contact.
Cross-channel opt-out enforcement. An opt-out in SMS implies opt-out across IVR, email, and other automated channels. The full cross-channel/cross-topic requirement was delayed until April 11, 2026, but smart teams are implementing it now.
NLU for messy opt-out language. People misspell things. They write "plz stop texting me" instead of "unsubscribe." An mPulse survey found ~80% of consumers were unaware of the changes, and 76% said they'd change their preference management if they knew one-channel opt-out removes all channels. Invest in natural language understanding to catch variants.
Healthcare Prospecting and Data Quality
Healthcare prospecting starts with NPI targeting - using the unique 10-digit National Provider Identifier assigned under HIPAA to segment physicians by specialty, location, institutional affiliation, and clinical focus. It's the healthcare-native equivalent of firmographic filtering.
Healthcare lists decay brutally. Physician inboxes get hammered with ~30 spam messages per day post-COVID, and workforce churn is accelerating - roughly 1 in 3 physicians intend to reduce hours, and 1 in 5 plan to leave their practice entirely. Your "verified" list from three months ago is already degrading.
Send in small batches and strip salesy signals - excess punctuation, emojis, and long unbroken text blocks trigger healthcare spam filters faster than in other verticals. This is where the biggest ROI in your stack lives. Not in the sequencing tool. In the data layer. In a vertical where your total addressable market might be a few thousand contacts, every bounced email hurts disproportionately, and a 7-day data refresh cycle (like Prospeo's) versus the industry-standard 6-week cycle can be the difference between a healthy sender reputation and a blacklisted domain.
If you're seeing bounces climb, start with email bounce rate diagnostics and then work backward into list sourcing and verification.
In a vertical where your entire TAM might be 4,000 hospital systems, every bounced email burns sender reputation you can't rebuild. Prospeo's 7-day data refresh cycle and 98% email accuracy keep your healthcare outreach hitting real inboxes - not spam traps. At $0.01 per verified email, protecting your domain costs less than a single compliance review.
Stop torching your sender domain on decayed physician data.
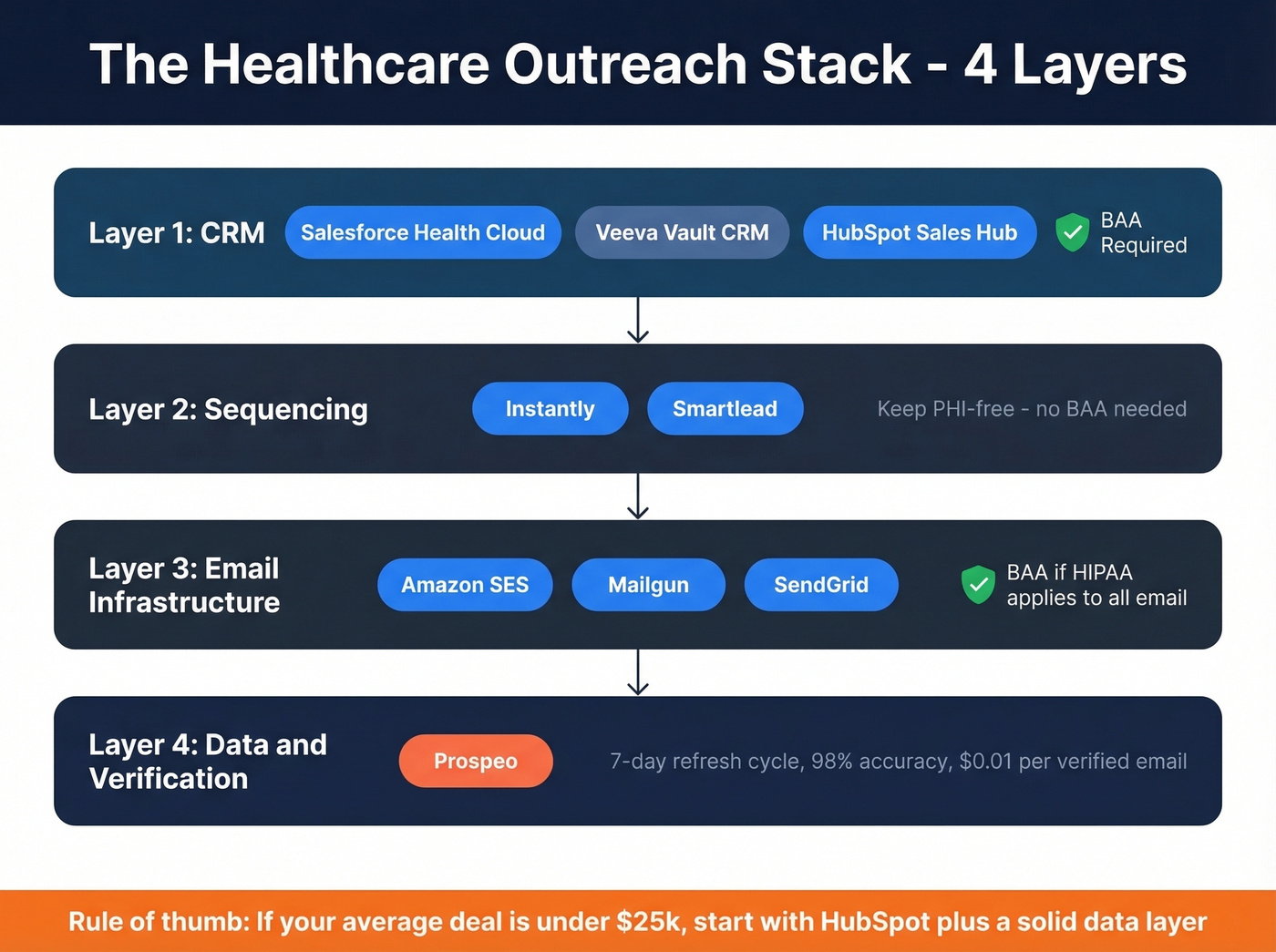
Building Your Outreach Stack
The stack has four layers. Here's what realistic pricing looks like.
| Layer | Tool | Price | HIPAA Status |
|---|---|---|---|
| CRM | Salesforce Health Cloud | ~$150-$300+/user/mo | Yes (BAA) |
| CRM | Veeva Vault CRM | ~$120-$150/user/mo | Yes (life sciences) |
| CRM | HubSpot Sales Hub | ~$20-$150/user/mo | Yes (with config) |
| Sequencing | Instantly | Starts at $37/mo | N/A - no PHI |
| Sequencing | Smartlead | ~$39-$99/mo | N/A - no PHI |
| Email Infra | Amazon SES | $0.10/1K emails | Yes (AWS BAA) |
| Email Infra | Mailgun | Custom (enterprise BAA) | Yes |
| Email Infra | SendGrid | Custom (Pro+/enterprise BAA) | Yes |
CRM depends on your org size. Veeva Vault CRM holds ~80% of the global pharma field sales CRM market, with hundreds of compliance features and full offline iPad support. It's the right choice for a 5,000-rep pharma organization. For a 10-person healthtech team? Overkill. Salesforce Health Cloud or HubSpot is the move.
Sequencing should be PHI-free by design. Don't put patient data in your outreach sequences - ever. Standard tools like Instantly and Smartlead work fine without a BAA. Enterprise platforms like Outreach and Salesloft work too; just keep them PHI-free unless you have a signed BAA in place.
Email infrastructure only matters if your org applies HIPAA rules to all outbound email. If so, route through Amazon SES with a signed BAA and CloudTrail logging.
Let's be honest: if your average deal size is under $25k, you probably don't need Salesforce Health Cloud or Veeva. HubSpot's free CRM plus a solid data enrichment layer will outperform an expensive CRM filled with stale contacts.
To keep the stack from turning into a mess, follow a simple lead generation workflow and document who owns each handoff.
Healthcare buying committees have 22 decision-makers. You need verified direct emails for every one of them - not generic info@ addresses that bounce. Prospeo's 300M+ profiles with 30+ filters let you segment by title, department, and company size so your sequences reach the CMO, the CISO, and the procurement lead in the same account.
Map the full buying committee with data that actually connects.
Choosing the Right Engagement Channels
A 14.7-month sales cycle with 22 stakeholders means you're not running a single-threaded drip. You're multi-threading across the buying committee - the CMIO, the VP of IT, the compliance officer, the department head who'll champion your product internally.
If you need a framework for this, borrow from account-based selling best practices and treat each hospital system like a mini-market.

Message fatigue in healthcare is real and measurable. A JAMA study of 428,000+ adults found that recipients getting more than 10 automated messages per year were significantly more likely to opt out, and those receiving 20+ were 3x more likely to opt out than those getting just 2. That's patient data, not B2B, but the principle transfers. For healthcare B2B, aim for 6-8 touches per quarter across channels rather than hammering email alone.
Belkins reports lead-to-appointment conversion rates of 4.2%-13.8% across ~100 B2B healthcare campaigns. The gap comes down to targeting quality and message relevance - not send volume.
Forget AI-written emails for healthcare prospects. Physicians smell templates. Use AI for research, targeting, and timing - identifying which committee members are active, what their institution just published, when budget cycles open - but write the first touch yourself. A two-sentence email referencing their department's recent EHR migration will outperform any AI-generated "thought leadership" template. We've tested this across dozens of healthtech campaigns, and the personalized two-sentence approach consistently doubles reply rates compared to templated sequences.
If you want a baseline structure for follow-ups, adapt proven sales follow-up templates to healthcare language (outcomes, risk, validation).
Reaching Prospects Working Remotely
The shift to remote and hybrid work hasn't bypassed healthcare administration. While clinicians are on-site, the IT directors, compliance officers, and procurement leads on your buying committee are often working from home two to three days a week.
Adjust your sequences accordingly: schedule calls for in-office days (typically Tuesday through Thursday), and lean on email and async touches for the rest of the week. Short video messages can cut through inbox noise when a prospect isn't sitting next to a desk phone.
If your team is doing more virtual selling, tighten up your remote sales meeting tips so calls don’t drift.
Event Marketing for Healthcare Sales
Healthcare conferences - HIMSS, HLTH, ViVE - remain high-value touchpoints, but the ROI comes from what you do before and after the event, not from staffing a booth.
Start targeted outreach 4-6 weeks before the conference to confirmed attendees. You can win these events without a booth by running a focused pre-event email campaign, hosting a small dinner or roundtable, and scheduling 1:1 meetings in advance. Reference a specific session or speaker the prospect is attending - it signals you've done your homework, not just scraped the attendee list. Pair that pre-event personalization with disciplined post-event follow-up within 48 hours, and you'll outperform teams that spent $50k on booth space.
What to Automate vs. Keep Human
Most healthcare teams are under-automating, not over-automating. Compliance fear causes paralysis. The answer isn't "don't automate" - it's automate correctly.
Automate: data enrichment and email verification, follow-up scheduling after initial engagement, CRM logging and activity tracking, engagement tracking (opens, clicks, replies), and meeting summaries synced to CRM.
Keep human: first-touch emails to senior clinicians, compliance reviews of outreach content, clinical conversations and product demos, procurement negotiations, and relationship-building with internal champions.
McKinsey's State of AI report shows 88% of organizations now use AI regularly in at least one business function, but only 39% attribute any EBIT impact - and most of those say it's less than 5% of EBIT. AI and automation create efficiency, but the revenue impact comes from how humans use that freed-up time. In healthcare sales, that means spending less time on data hygiene and more time building relationships with the 22 people who need to say yes.
One thread on r/b2bmarketing about selling to small medical groups put it well: the reps who close deals are the ones who show up knowing the practice's specific pain points, not the ones who send the most emails. Automation should buy you the time to do that research.
If you're standardizing this across the org, document it as sales process optimization so new reps don’t reinvent the wheel.
Retargeting Previous Buyers
One of the highest-ROI motions in healthcare is retargeting previous buyers.
Hospital systems that purchased one product are significantly more likely to buy adjacent solutions - they've already cleared your vendor risk assessment, your BAA is on file, and procurement knows your paperwork. Build a dedicated sequence for past customers entering new budget cycles or expanding to new departments. This re-engagement motion consistently outperforms cold outreach by 3-5x on reply rates in our campaigns. Skip this if you don't have at least 20 past customers to work with; below that threshold, manual outreach to each account is more effective than building a dedicated automated sequence.
FAQ
Is cold email to physicians HIPAA-compliant?
Cold outreach using business contact information - name, work email, title - isn't a HIPAA violation. PHI is the trigger, not the act of emailing. Keep patient data, clinical records, and insurance details completely out of your sequences, and you're operating in a compliant PHI-free workflow. Most compliance teams overcorrect here, stalling pipeline for months over risks that don't apply.
How often should I email healthcare prospects?
Opt-out rates spike sharply after 10+ automated messages per year, based on the JAMA study of 428,000+ adults referenced above. For healthcare B2B, aim for 6-8 touches per quarter spread across email, phone, and direct mail. Quality of targeting and message relevance matter far more than send volume in a small-TAM vertical.
What's the best CRM for healthcare sales?
Salesforce Health Cloud is the strongest all-around choice for teams needing HIPAA compliance baked in. Veeva dominates pharma field sales but is overkill for most healthtech startups. HubSpot works well for teams under 20 reps with deal sizes below $30k - pair it with a strong data enrichment layer and you won't miss the enterprise features.
What's a reliable free tool for verifying healthcare email lists?
Prospeo's free tier includes 75 verified emails per month with 98% accuracy - enough to validate a small healthcare list before you commit to a paid plan. Other options like Hunter offer 25 free searches monthly but cap enrichment. For teams running real campaigns against a finite TAM, accuracy and refresh frequency prevent the domain damage that bad data causes.
How does healthcare outreach compare to financial services?
Healthcare shares DNA with financial services sales - both involve heavy regulation, long cycles, and buyers skeptical of generic pitches. The key difference is TAM size: healthcare buying committees are larger (22 stakeholders on average), and total target accounts are often smaller, making data quality and deliverability even more critical. Teams experienced in regulated-industry outreach will recognize the compliance-first mindset, but healthcare's multi-stakeholder complexity is in a class of its own.