Healthcare Buyer Intent Signals: What to Track, Score, and Act On in 2026
Your SDR just sent 200 cold emails to hospital CIOs. Half bounced. A quarter hit the wrong person. Meanwhile, three health systems in your territory filed Certificate of Need applications, two announced Epic migrations, and one posted five clinical informatics roles in a single week.
Your team missed all of it.
Healthcare buying committees average 22 decision-makers, deals take 14.7 months from first touch to signature, and 68% stall when stakeholders fall out of alignment. If you're not tracking the right healthcare buyer intent signals, you're prospecting blind into the most complex B2B market on the planet.
The Quick Version
Three signals to watch right now:
- EHR migrations - Centralus Health moving to Epic, UK HealthCare preparing for a 2026 go-live, Huntsville Hospital Health System deploying Oracle Health Foundation EHR
- CMS 2026 rule changes - IPPS final rule CMS-1833-F, PFS conversion factor at $33.59 (+3.77%) for qualifying APMs / $33.42 (+3.26%) for nonqualifying, IPO list phase-out
- Leadership hires - a new CIO, CMIO, or VP of Population Health means vendor re-evaluation within six months
A free monitoring stack covers 80% of what matters: CMS.gov rule pages, Becker's Hospital Review EHR category, state CON databases, and job boards.
The gap most teams ignore? Intent without verified contacts is an expensive dashboard you can't act on.
What Are Healthcare Buyer Intent Signals?
In standard B2B, buyer signals are behavioral cues - pricing page visits, content downloads, review-site comparisons - that suggest a company is actively evaluating solutions. Healthcare adds two layers that don't exist in most industries.
First, regulatory and compliance intent. When CMS publishes a rule that changes reimbursement rates or mandates new price transparency requirements, it creates budget pressure across thousands of hospitals simultaneously. Second, clinical operations intent. EHR migrations, telehealth expansions, and value-based care shifts signal technology buying windows that last 12-24 months. Layer these on top of standard engagement, research, and hiring signals, and you've got a far richer - and more complex - set of buying indicators.
In a market where U.S. healthcare spending hit $4.8 trillion, the stakes for reading these signals correctly are enormous.
The 9 Signals That Matter Most
1. EHR Migrations
This is the single strongest buying signal in healthcare IT. Centralus Health is rolling out Epic, UK HealthCare is preparing for a 2026 go-live, and Huntsville Hospital Health System is deploying Oracle Health Foundation EHR. Each migration opens a 12-24 month window for adjacent vendors - integration middleware, training platforms, data migration tools, cybersecurity layers, and analytics overlays. The consensus across healthcare sales communities on Reddit is that EHR migration announcements are the single most actionable prospect signal you can track. We've seen teams build entire quarterly pipelines around a single health system's Epic go-live.
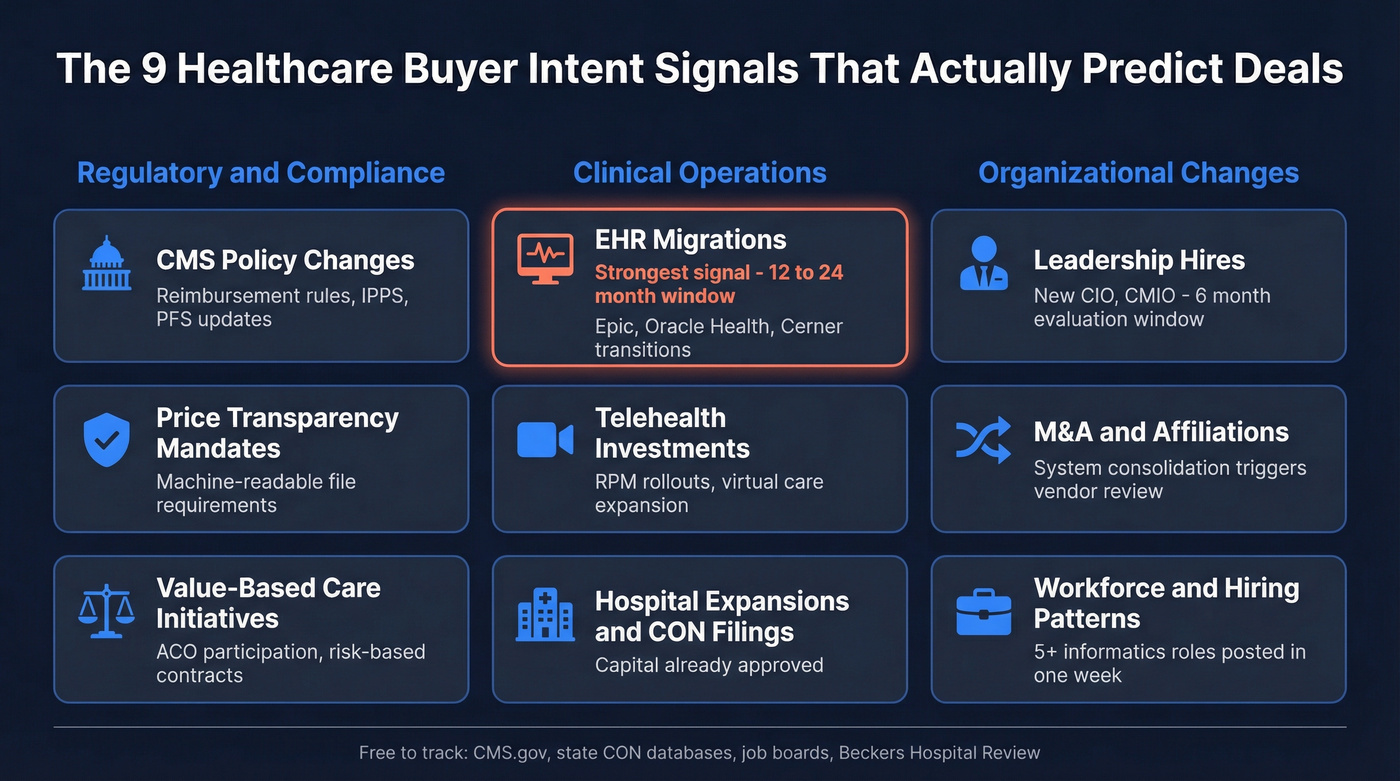
2. CMS Policy Changes
How big can the budget impact get? Medicare spending on skin substitutes alone jumped from $252M in 2019 to over $10B by 2024 - and CMS is now rewriting the reimbursement rules around it. The FY 2026 IPPS final rule (CMS-1833-F) touches reimbursement, interoperability, electronic prescribing, real-time prescription benefit, and electronic prior authorization. The PFS conversion factor jumped to $33.59, up 3.77% from 2025 for qualifying APMs. CMS is also phasing out the Inpatient Only list, removing 285 procedures in 2026. Every one of these changes triggers budget conversations - free to track and highly predictive.
3. Price Transparency Mandates
Starting January 1, 2026, hospitals must publish 10th, 50th, and 90th percentile allowed amounts in machine-readable files when negotiated charges are algorithm- or percentage-based. Compliance teams are scrambling. If you sell anything adjacent to price transparency, this is your moment.
4. Hospital Expansions and CON Filings
When a health system files a Certificate of Need application, budget is unlocked. State CON databases are free and public - check them monthly. A new surgical wing means procurement cycles for everything from IT infrastructure to clinical equipment. These filings are among the clearest buying indicators because they represent capital already approved.
5. Leadership Hires
Here's the thing: I've watched teams ignore this signal and regret it for quarters. A new CIO or CMIO wants to put their stamp on the technology stack. The six-month window after a C-suite hire is the most reliable vendor-evaluation trigger in healthcare. Pairing this signal with verified decision-maker contacts is what turns awareness into booked meetings.
6. Value-Based Care Initiatives
New ACO participation, population health investments, and shifts toward risk-based contracts all signal technology buying. Health systems moving deeper into value-based care need analytics, care coordination, and patient engagement platforms - and they need them fast.
7. Telehealth Investments
Platform expansions, remote patient monitoring rollouts, and virtual care infrastructure upgrades continue to drive spending. When a health system announces a telehealth expansion, adjacent vendors should already be in the pipeline.
8. M&A and Affiliations
Two health systems merge. They don't keep two EHRs, two revenue cycle platforms, and two cybersecurity stacks. Monitor EDGAR for publicly traded healthcare companies and health-system-related debt/financing disclosures, and use trade press for nonprofit affiliations.
9. Workforce and Hiring Patterns
Five or more clinical informatics roles posted in a single week? An EHR project is underway. A burst of data engineering hires? Analytics infrastructure is being built. Job postings are free, public, and surprisingly predictive.
Signal-to-Stakeholder Map
With 22-person buying committees, you can't just reach the CIO and hope for the best. Different signals activate different stakeholders, and you need to multi-thread across all of them.
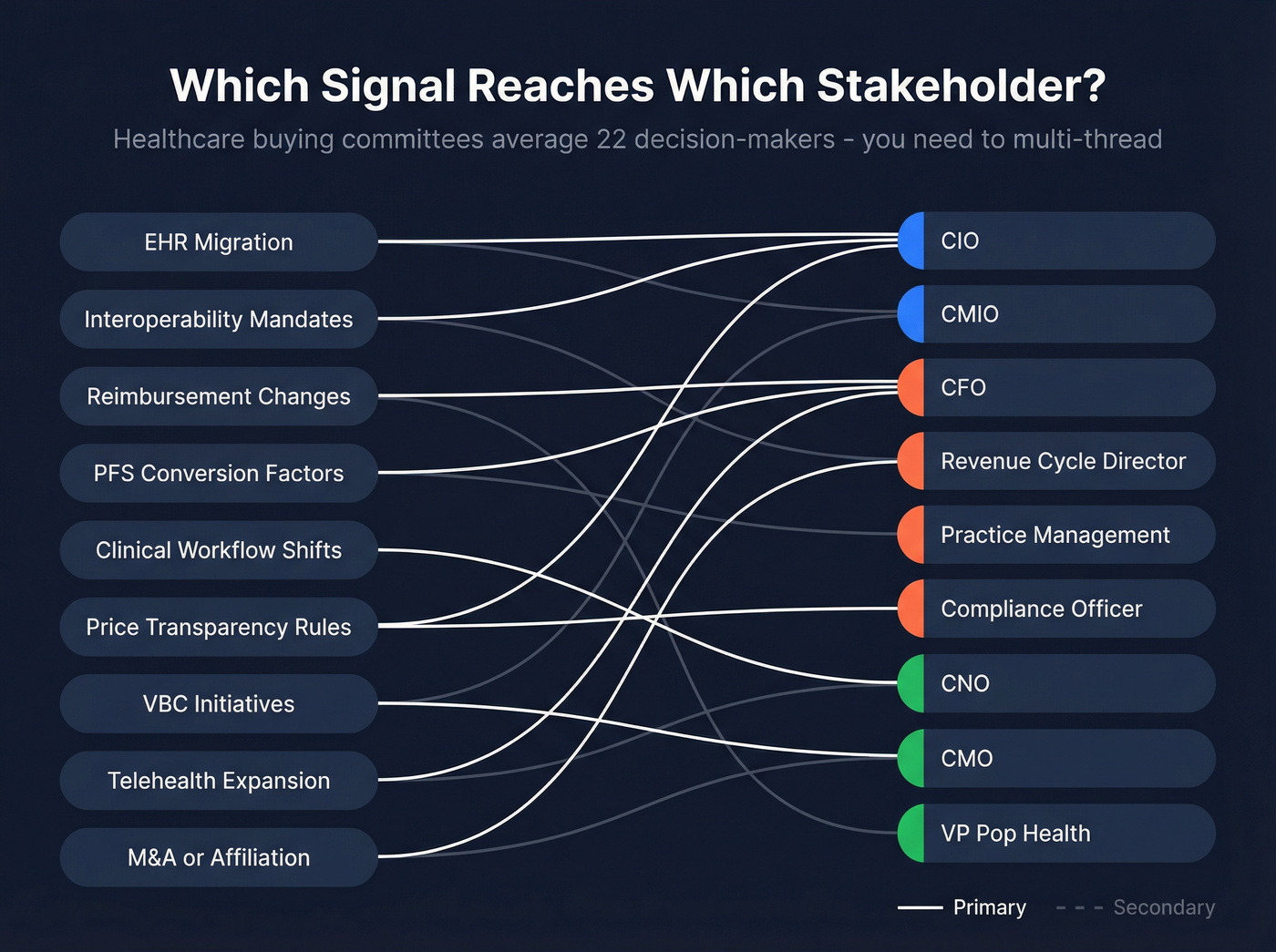
| Signal | Primary Stakeholder | Secondary |
|---|---|---|
| EHR migration | CIO | CMIO |
| Interoperability mandates | CIO | Compliance Officer |
| Reimbursement changes | CFO | Revenue Cycle Dir. |
| PFS conversion factors | CFO | Practice Mgmt. |
| Clinical workflow shifts | CMIO | CNO |
| Price transparency rules | Compliance Officer | CFO |
| VBC initiatives | VP Pop Health | CMO |
| Telehealth expansion | CIO | CMO |
| M&A / affiliation | CIO | CFO |
Mapping each signal to the right contact is what separates teams that close from teams that stall at "interested but can't get alignment."
You just mapped 9 intent signals to the right stakeholders. But signals without verified contact data are just dashboards you can't act on. Prospeo gives you 98% accurate emails and 125M+ verified mobile numbers for healthcare CIOs, CMIOs, and CFOs - so when a health system files a CON application or announces an Epic migration, you're already in their inbox.
Turn healthcare intent signals into booked meetings for $0.01 per email.
How to Score Intent in Healthcare
Generic lead scoring doesn't work here. Email opens are meaningless after Apple's Mail Privacy Protection changes, and a pricing page visit from a 25-bed critical access hospital shouldn't score the same as one from a 15-hospital system.
| Signal | Points | Rationale |
|---|---|---|
| EHR migration announced | +30 | Creates budget + urgency |
| CMS rule affects their line | +25 | Regulatory pressure |
| CON filing / capital approval | +25 | Budget unlocked |
| Leadership hire (CIO/CMIO) | +20 | Vendor re-evaluation |
| Topic surge (intent provider) | +15 | Active research |
| Pricing page visit | +15 | Direct evaluation |
| Review-site comparisons | +10 | Shortlisting |
| Email open | +2 | Unreliable - de-emphasize |
| Bounced email | -25 | Bad data, penalize hard |
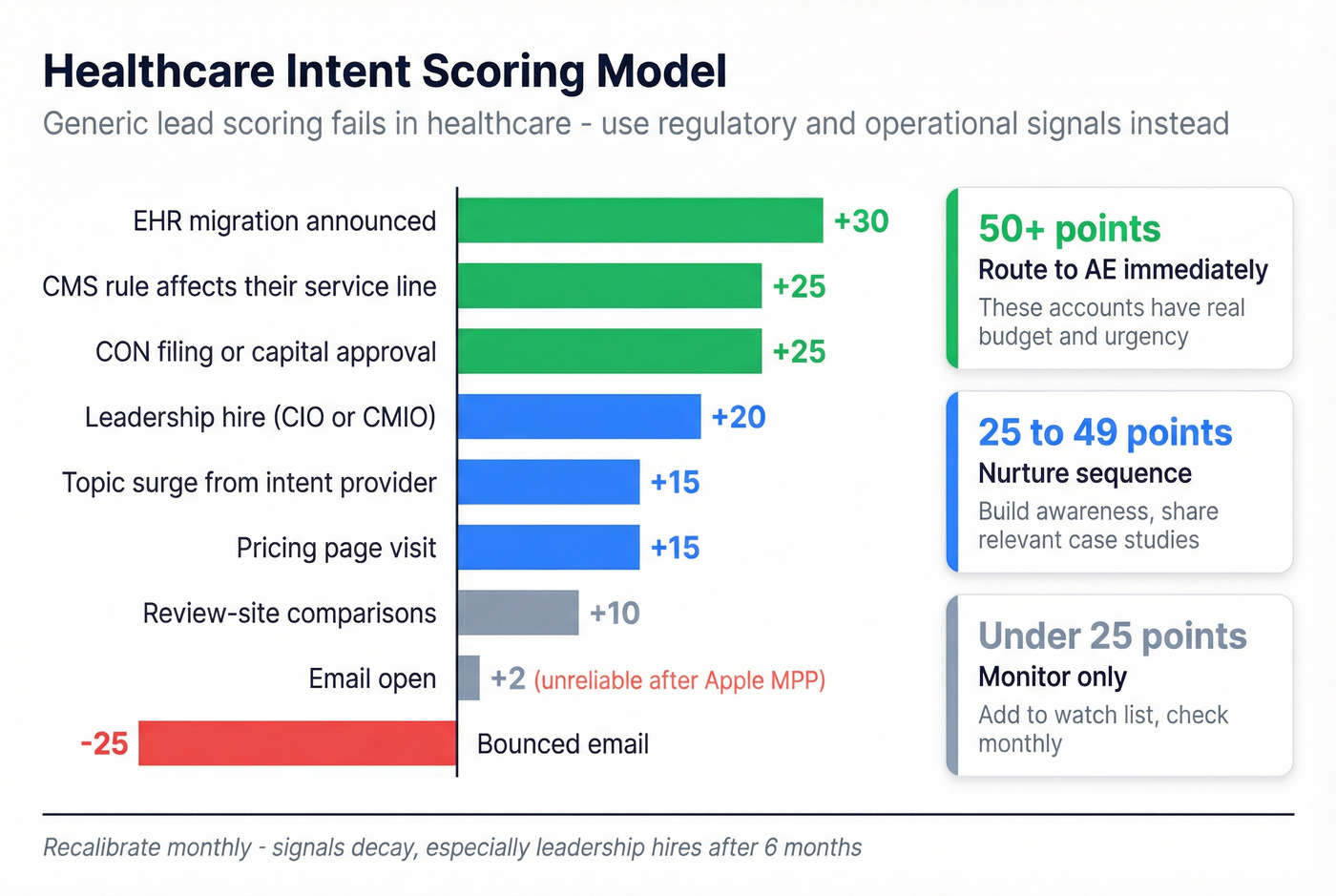
Route 50+ point accounts to an AE immediately. Nurture 25-49. Monitor everything else. Recalibrate monthly - signals decay, especially leadership hires after the six-month window closes.
Let's be honest: most healthcare sales teams over-invest in digital intent signals and completely ignore the regulatory calendar. A CMS final rule affecting your buyer's service line is worth more than a thousand topic surges - and it's free to track. The real problem isn't that intent data is overrated. It's that teams track the wrong signals - webinar registrations and email opens - instead of regulatory and operational triggers that actually predict spend.
Budget timing matters too. Many health systems operate on a July 1 fiscal year, with capital budget planning happening 6-9 months before. An EHR migration announced in January means the budget was likely approved the previous spring. Time your outreach to the planning cycle, not just the announcement.
Where to Monitor These Signals
You don't need a $100K platform to track most of this.
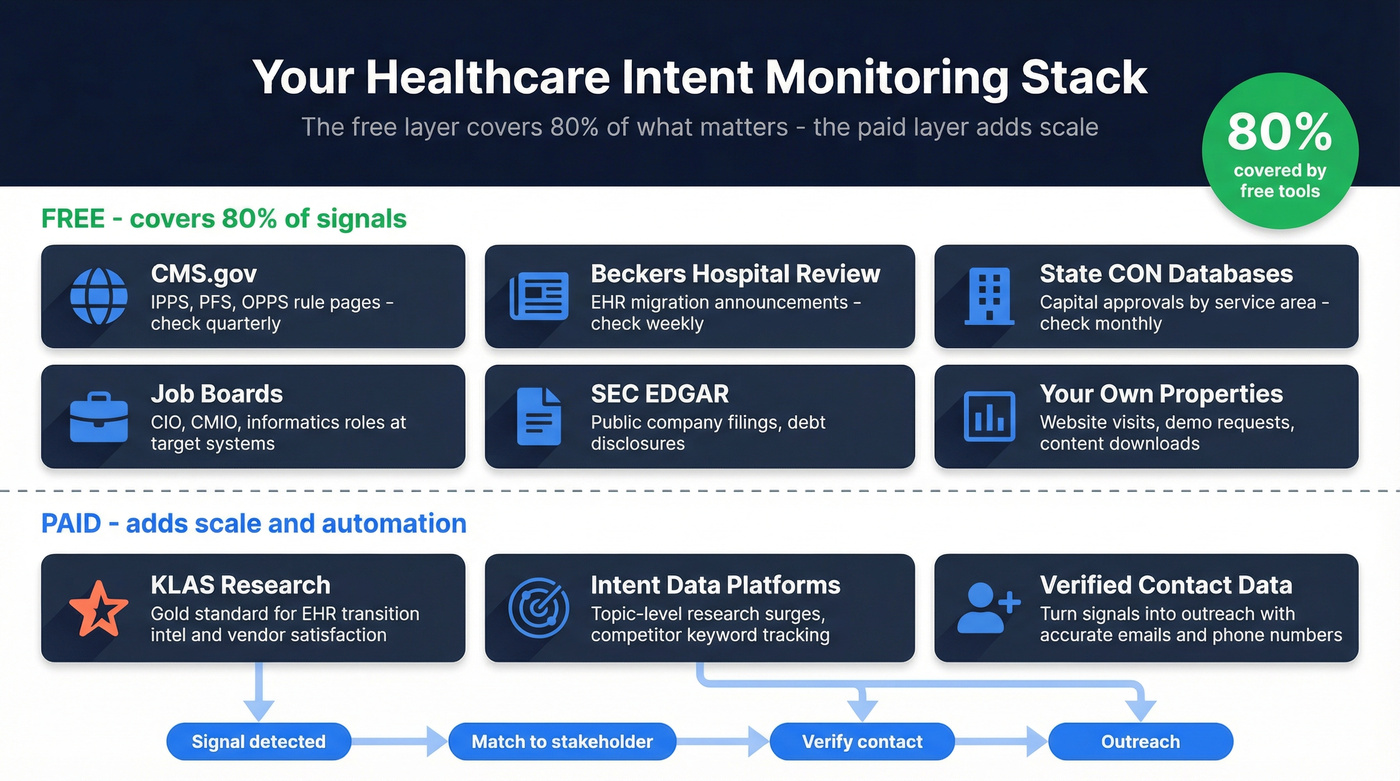
- CMS.gov - IPPS, PFS, and OPPS/ASC rule home pages. Check quarterly when final rules drop.
- Becker's Hospital Review - EHR category pages for named migration announcements. Check weekly.
- KLAS Research - Paywalled, but the gold standard for EHR transition intelligence and vendor satisfaction.
- State CON databases - Free, state-by-state. Search for your target accounts' service areas.
- Job boards - Filter by title at target health systems. CIO, CMIO, VP Population Health, Clinical Informatics.
- SEC EDGAR - Free filings for publicly traded healthcare companies and health-system-related financing disclosures.
- Intent data platforms - For topic-level research surges across the web. These capture signals like competitor keyword research and category-level content consumption.
- Your own properties - First-party data from website visits, demo requests, and content downloads remains the highest-fidelity source.
The free stack covers roughly 80% of the signals that matter most. The paid layer adds scale and automation.
What Healthcare Intent Data Costs
Most teams assume they need an enterprise intent platform to get started. They don't. But if you want automated topic-surge detection across thousands of accounts, here's what you're looking at.
| Provider | Annual Cost | Notes |
|---|---|---|
| Prospeo | Free tier; ~$0.01/email | 15K topics + 300M+ professional profiles |
| Bombora | $25K-$80K | 400+ healthcare topics, annual |
| Demandbase | $40K-$120K | Full ABM orchestration |
| 6sense | $35K-$150K+ | Enterprise, modular pricing |
| ZoomInfo | $7.2K-$36K | Intent is an add-on module |
| G2 Buyer Intent | $10K-$87K+ | Review-site intent only |
Budget 15-25% above the license price for implementation, topic configuration, and CRM integration. That's the hidden cost most vendors don't mention upfront.
Half the most valuable healthcare signals are free - CMS rules, CON filings, leadership hires. The expensive part isn't knowing who's in-market. It's reaching the right person once you know.
From Intent Data to Booked Meetings
Intent data tells you which health system is evaluating interoperability solutions. It doesn't give you the CMIO's verified email.
And with 22-person buying committees, you need the CIO, CFO, CMIO, compliance officer, and VP of Population Health - all with working contact data. We've seen teams spend $40K+ on an ABM platform, identify 50 in-market accounts, and then stall because their contact database hasn't been refreshed in six weeks.
Prospeo closes this gap. With 143M+ verified emails at 98% accuracy, 125M+ verified mobile numbers, and a 7-day data refresh cycle, it turns "this health system is in-market" into "here's the CMIO's verified email and the CFO's direct dial." Intent data across 15,000 Bombora-powered topics is built in, so you can identify in-market accounts and pull verified contacts without stitching together three separate tools.
Healthcare buying committees average 22 stakeholders. Multi-threading across CIOs, compliance officers, and CFOs means you need direct dials that actually connect. Prospeo's 30% mobile pickup rate is 3x the industry average - and with 30+ filters including job changes and department headcount, you'll know the moment a new CMIO lands and be first to reach them.
Stop losing deals to misaligned stakeholders you never contacted.
How Healthcare Signals Compare to Other Verticals
The scoring framework above is built for healthcare, but the underlying logic transfers. In logistics, teams track fleet expansion announcements, warehouse lease filings, and TMS RFPs. In manufacturing, it's capital equipment orders, plant expansions, and ISO certification timelines. Banking has its own version - branch technology refreshes, core banking platform migrations, and regulatory compliance deadlines.
What makes healthcare unique is the regulatory layer and the sheer size of the buying committee. But the discipline of tracking observable behavior that predicts a purchase works everywhere. Skip this section if you're purely healthcare-focused - but for teams selling across verticals, the pattern recognition is worth internalizing.
FAQ
What's the difference between first-party and third-party intent data?
First-party intent comes from your own channels - website visits, email engagement, demo requests. Third-party intent comes from external networks like Bombora's 5,000+ B2B site cooperative, tracking research behavior across the broader web. Most healthcare teams need both: first-party is higher fidelity but lower volume, while third-party scales coverage but requires validation.
How long do healthcare intent signals take to convert?
Healthcare deals average 14.7 months from initial contact to closed deal. Strong signals like EHR migrations can compress this, but expect 6-12+ months from signal detection to signature even with high-priority triggers.
Is tracking healthcare buyer intent HIPAA-compliant?
B2B intent data tracks company-level research behavior, not patient data - no protected health information is involved. Avoid patient-level tracking, minimize data retention beyond what's operationally necessary, and make sure vendor data processing agreements are in place.
Which intent signals have the highest conversion rate?
EHR migration announcements and CMS policy changes affecting a specific service line are the strongest - they create budget and urgency simultaneously. Leadership hires at the CIO or CMIO level are a close third. Digital signals like whitepaper downloads add a useful layer, but regulatory and operational triggers remain more predictive.
What's a cost-effective way to start?
A free Prospeo tier paired with CMS.gov monitoring and Becker's Hospital Review covers the majority of actionable signals without any upfront spend. For teams scaling beyond that, layering in Bombora-powered intent data with verified contacts at ~$0.01/email replaces the need to stitch together a $50K+ intent platform and a separate contact database.