How to Pitch Doctors: Scripts, Frameworks, and What Physicians Actually Want to Hear
A surgeon walks out of the OR, pulls off gloves, and you've got 90 seconds before the next case. That window is your entire sales pitch to doctors. A single knee implant account runs $875K in annualized sales, and a Da Vinci Xi deal tops $2M - those seconds carry real weight.
We've watched reps blow six-figure accounts by opening with a feature dump in that window. Every training program teaches "build rapport, know your product, respect their time." You already know that. Here are the actual words.
What Physicians Actually Hate
The fastest way to lose a doctor is to sound like every other rep who walked in that day.
- "Doctor, tell me how you treat [condition]?" - The single worst opener, per physicians themselves. It feels like a trap. The doctor knows you're about to tell them they're wrong. Instead, quote a published article and ask if the authors' approach fits their patient population.
- Memorized scripts delivered on autopilot. Doctors communicate in one- to two-minute bites. They can smell a canned pitch from across the hallway.
- Canned closes. "Doctor, can I have your commitment today that you'll use my product on the next 20 patients?" This isn't a car dealership. Stop.
- Pushing through your call plan when the physician signals a different interest. This is by far the most common mistake. Listen first. Adjust second. Pitch third.
The Pitch Framework: Validate, Probe, Evidence, Close
Stop memorizing your pitch. Memorize your questions instead. The best-performing medical sales reps aren't walking encyclopedias of clinical trial data - they're the ones who ask better questions in the maybe three minutes they get.
Here's how it sounds when you're pitching a skeptical cardiologist:
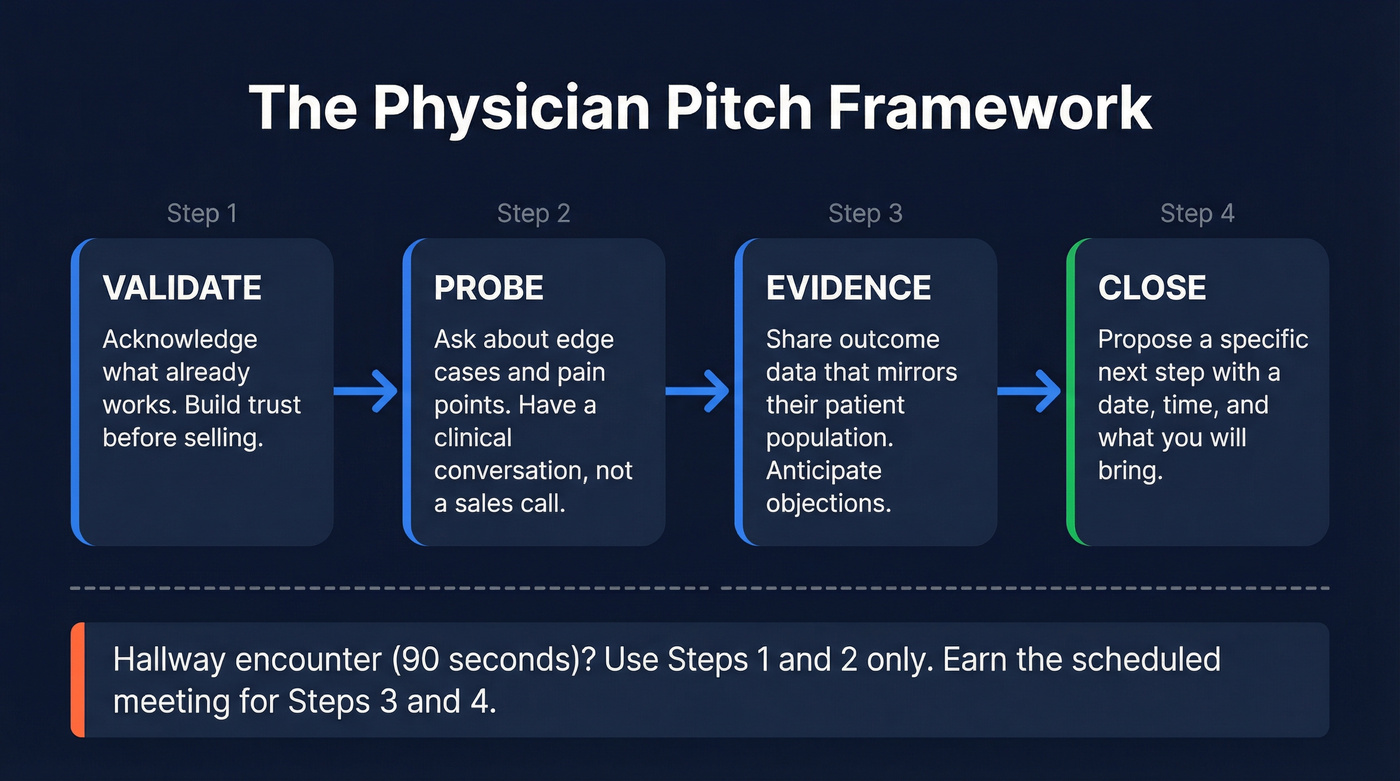
Step 1 - Validate the status quo. "Dr. Chen, your statin protocol clearly works for most patients. You shouldn't change what's effective." You're not selling yet. You're earning trust before anything else, and that distinction matters more than any data point you'll share later.
Step 2 - Probe for edge cases. "What about the patients who can't tolerate statins? The ones with muscle pain or liver enzyme issues - how are you managing those?" Now you're having a clinical conversation, not a sales call.
Step 3 - Evidence, framed around outcomes. "The five-year data looked at actual heart attacks and strokes, not just cholesterol numbers. 45% of trial patients had diabetes, 30% had moderate kidney problems - so the population mirrors what you're seeing." Anticipate the external validity question before they ask it.
Step 4 - Close on a specific next step. "Would next Thursday at 2 PM work? I know that's your research block - I can bring the subgroup analysis for your renal patients."
For a 90-second hallway encounter, compress to steps 1 and 2 only. Validate, probe, and earn the scheduled meeting where you deliver steps 3 and 4. The framework scales. The words change, the structure doesn't.
How Setting Changes Everything
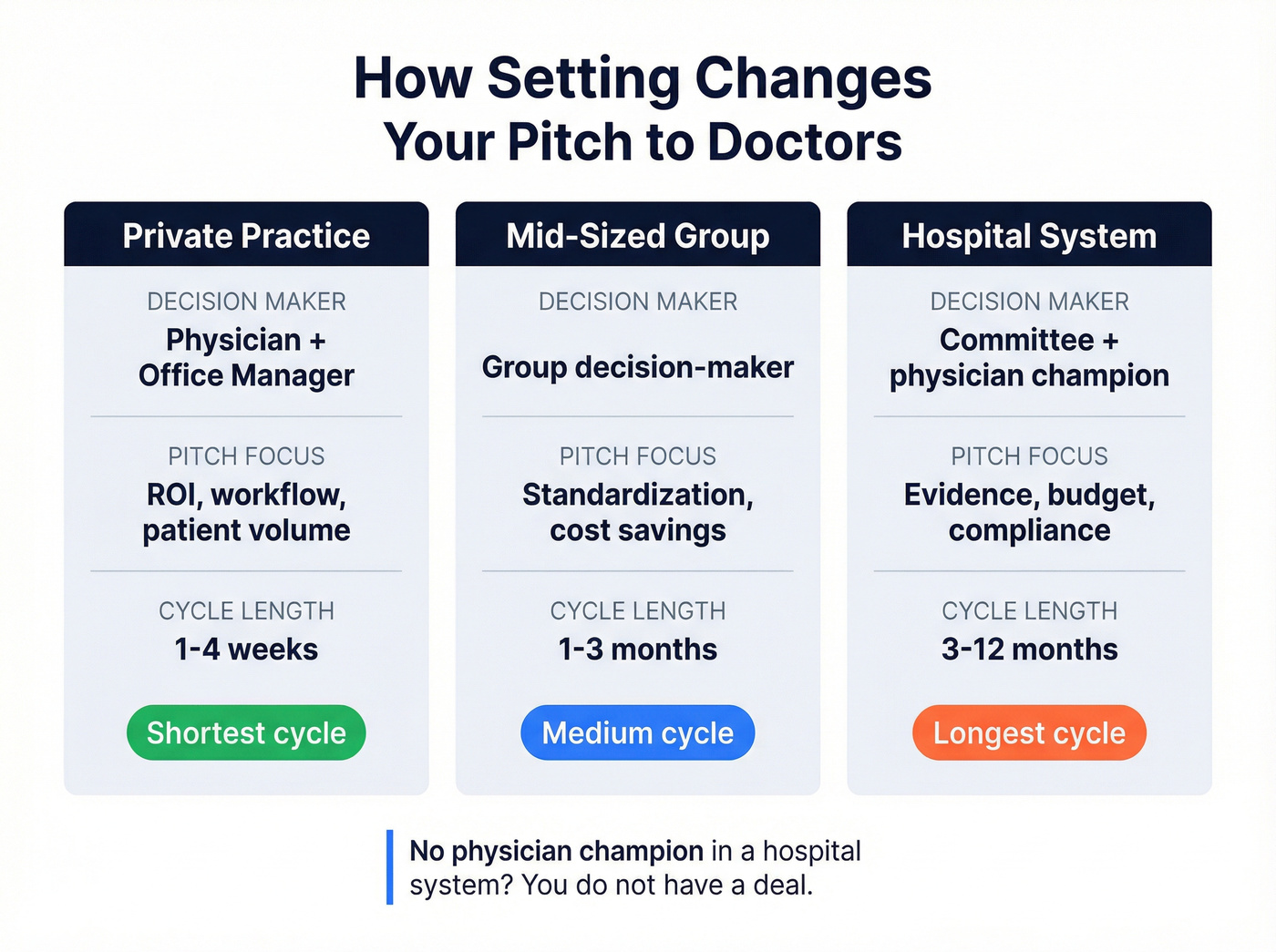
The physician isn't always the decision-maker. Where you're selling changes who you pitch and how.
| Setting | Decision-Maker | Pitch Focus | Cycle Length |
|---|---|---|---|
| Private practice | Physician + office mgr | ROI, workflow, volume | Short (1-4 weeks) |
| Mid-sized group | Group decision-maker | Standardization, savings | Medium (1-3 months) |
| Hospital system | Committee + champion | Evidence, budget, compliance | Long (3-12 months) |
In private practice, the doctor is a small business owner. The office manager is your second decision-maker - confirm their involvement early. Physicians respond to two things: better patient outcomes and metrics that make them look good. Time saved, volume handled, reimbursable revenue. Hit both or you're wasting their time.
Hospital systems are a different game entirely. Expect committee meetings and multiple stakeholders across supply chain, finance, and clinical departments. In surgical specialties, credible reps get invited into the OR to observe - that's where you build the clinical champion relationship that carries your deal through committee. If you're selling into a hospital system and you don't have a physician champion, you don't have a deal.
You nailed the hallway pitch. Now you need the follow-up email to land. Prospeo gives you verified emails for 300M+ professionals - including physicians - at 98% accuracy. Find the right doctor, enrich their profile with 50+ data points, and send that two-hour recap to a real inbox, not a bounce.
Stop guessing email addresses. Verify before you hit send.
Pitch Differences by Product Type
| Product Type | Deal Size Example | Visits/Day | Pitch Style |
|---|---|---|---|
| Capital equipment | Da Vinci Xi: $2M+ | 1-2 | Demo + committee |
| Implants | Knee: $875K/yr | 1-2 | OR presence + surgeon |
| Disposables | Gloves: $25K line | 5-10 | Volume + procurement |
| Diagnostics | Rapid tests: ~$150K/yr | 3-6 | Consultative + lab mgr |
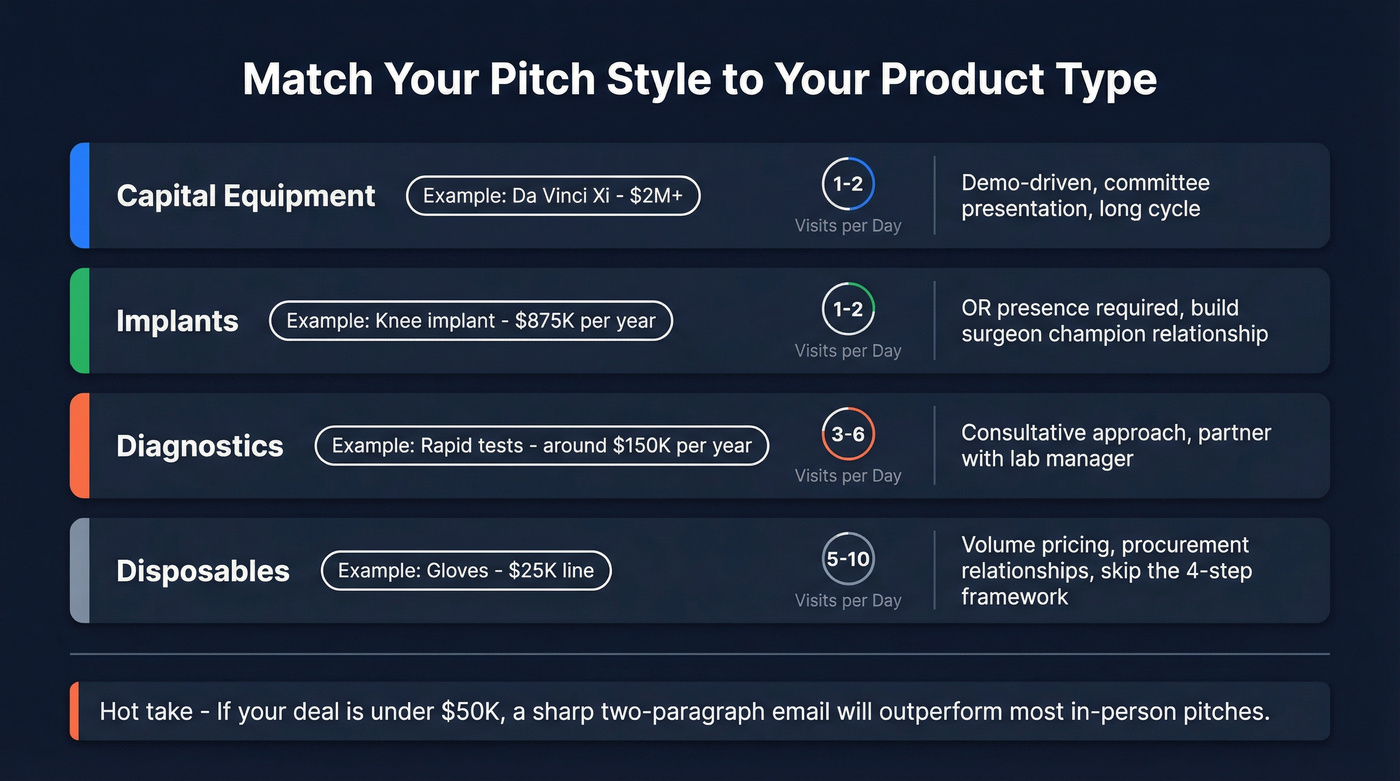
An implant rep scrubbing into multi-hour cases needs a fundamentally different approach than a disposables rep hitting five to ten offices. As one industry analysis from ConnectSx put it, "The era of pitching is over. The era of diagnosing has begun." Physicians and buying committees want to know how your solution saves time, reduces risk, and impacts downstream workflow and budget.
Here's the thing: if you're selling disposables at $25K a line, you don't need the four-step framework above. You need procurement relationships and volume pricing. Save the clinical storytelling for capital equipment and implant deals where the physician's clinical judgment actually drives the purchase.
Icebreakers and Gatekeeper Strategy
The gatekeeper isn't your enemy - they're your first sale. In our experience, the gatekeeper relationship is what separates closers from door-knockers.

A script that works: "Hi, I'm [name] with [company]. I have a quick update on [specific clinical topic] for Dr. [name] - is there a good time to catch them for two minutes this week, or should I leave materials with you?" Brief. Respectful. Specific.
The office manager controls the calendar. Bring them value - workflow insights, patient volume data, anything that makes their job easier. We've seen reps build entire accounts through the office manager relationship alone, especially in private practice settings where the office manager handles purchasing, scheduling, and vendor relationships all at once. If you need more options, borrow lines from what to say to get past the gatekeeper.
The Follow-Up That Lands
Your pitch doesn't end when you walk out. It ends when the doctor takes action.
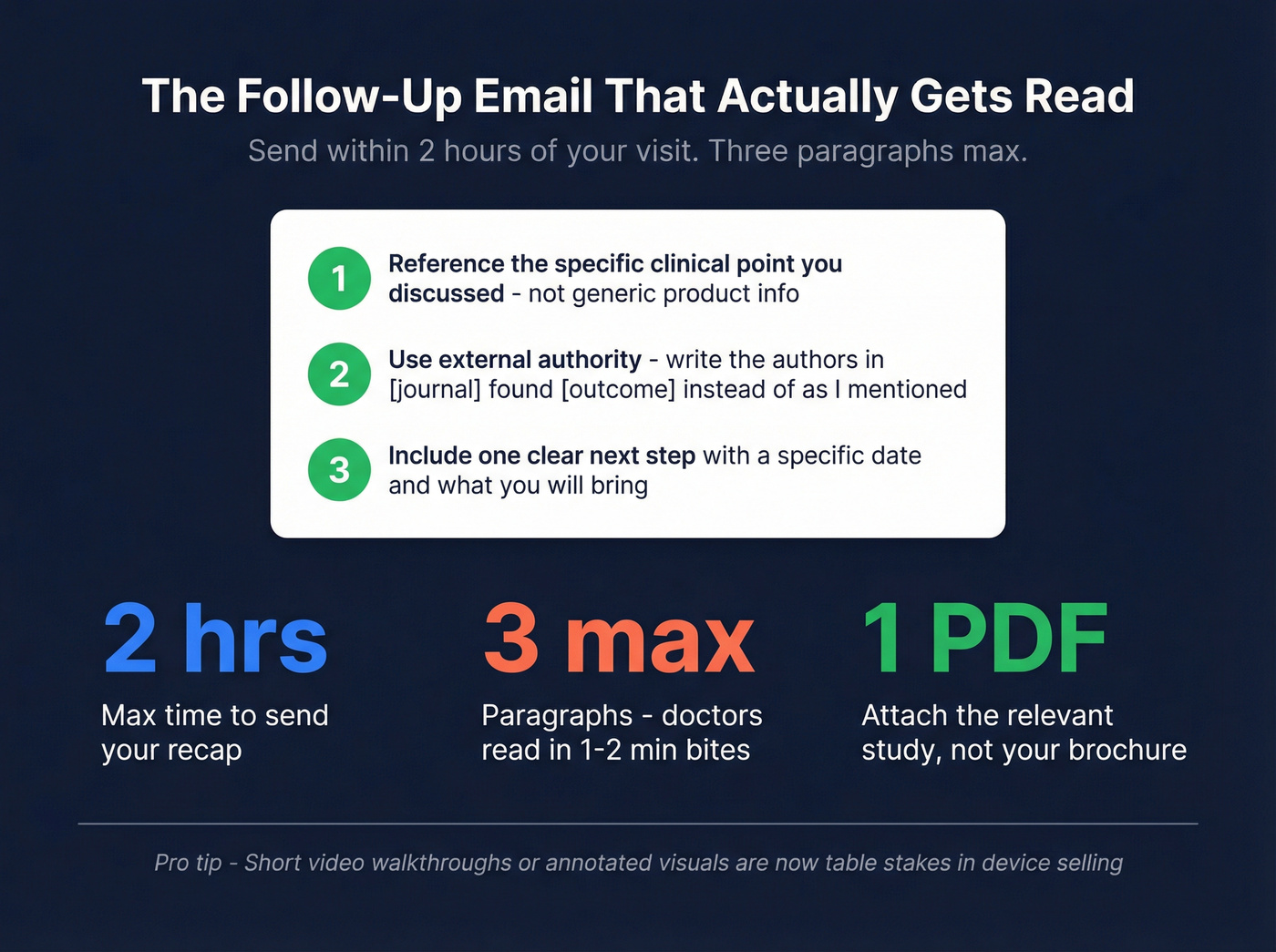
Send a recap email within two hours. Reference the specific clinical point you discussed, attach the relevant study, and include one clear next step. Use external authority - instead of "as I mentioned," write "the authors in [journal] found [outcome] - here's the PDF." Short video walkthroughs or annotated visuals attached to your recap are now table stakes in device selling, because buyers increasingly consume clinical content asynchronously. Three paragraphs max. Doctors read email in the same one- to two-minute bites they give you in person.
If you want a tighter structure, use a proven sales email structure and keep your ask aligned with how to ask for a meeting via email.
Before your next visit, run the physician through Prospeo's enrichment to pull 50+ data points you can use to personalize your opening line and skip the questions doctors hate. (If you're building a repeatable workflow, start with data enrichment for cold email.)
A hot take from our team: if your deal size is under $50K, you probably don't need a 10-minute sit-down with the physician. A verified email, a sharp two-paragraph recap, and a single compelling data point will outperform most in-person pitches. Healthcare sales is moving async faster than most reps realize, and the consensus on r/sales backs this up - reps who nail the email follow-up consistently outperform the ones grinding for face time. If you're sending volume, protect deliverability with an email deliverability checklist and validate lists with an email checker tool.
Skip the 10-visit courtship if you're selling sub-$50K deals. Your time is better spent on email precision than lobby waiting.
Selling into hospital systems means reaching multiple stakeholders - the surgeon champion, the office manager, procurement, and the committee. Prospeo's 30+ search filters let you map the entire buying committee by department, title, and facility, then pull verified emails and direct dials for each contact at $0.01 per email.
Map the full buying committee before your competitor gets a single meeting.
FAQ
How long do you get with a doctor during a sales pitch?
Unscheduled drop-ins typically give you 1-3 minutes. Scheduled lunch-and-learns run 10-20 minutes. Plan your core message for 90 seconds - anything beyond that is a bonus.
What's the biggest mistake reps make when pitching physicians?
Leading with product features instead of asking questions. Doctors hear the same memorized scripts daily. The reps who listen and probe for specific pain points earn the follow-up meeting. Features come later, after you've earned attention.
How should you reach out to a physician for the first time?
Pull their publication history, check recent conference presentations, and find a verified email. Lead with a clinical insight relevant to their specialty - not a product pitch. The goal of your first touch is to earn a conversation, not close a deal.