B2B Healthcare Marketing: What Generic Guides Won't Tell You
Your CEO just told you the company's going after health systems. You've got 90 days to build pipeline. You pull up every guide on B2B healthcare marketing, and they all say the same thing: build trust, publish thought leadership, stay compliant. Cool. None of them tell you how health systems actually buy, who's in the room, or what procurement wants before they'll even agree to a first call.
Look, selling into healthcare isn't "hard" because clinicians are skeptical. It's hard because the buying process is designed to reduce risk, and marketing that doesn't respect that reality gets filtered out fast.
We've tested this across outbound, events, and ABM plays. The teams that win don't just "create content." They engineer the deal.
What You Need (Quick Version)
- Average B2B CPL: $377 (healthtech SaaS ~$130; medical equipment $609)
- Conversion rate: 3-7% (sanity-check against your average lead conversion rate)
- Sales cycle: 6-12 months
- Healthy LTV:CAC ratio: >= 3:1
The playbook that works: ABM + compliance-first positioning + buying committee mapping. Everything else is noise.
Healthcare Buying Committee Map
Stop writing for "providers." That word flattens 6-10 distinct stakeholders into one useless persona, and it leads to generic messaging that doesn't land with anyone.

| Role | Example Titles | Priority | Content to Provide |
|---|---|---|---|
| Economic Buyer | CEO, CFO, Procurement Director | TCO/ROI, margin protection | Business cases, CFO metrics |
| Clinical Buyer | CMO, CNO, CMIO, Department Chief | Outcomes, workflow fit, burnout | Peer-reviewed results, pilots |
| Technical Buyer | CIO, VP Apps, IT Governance | Security, Epic/Cerner integration | Architecture docs, SOC 2, sandbox |
| Champion | End users, clinical staff | Time savings, usability | Workflow demos, quickstart guides |
| Gatekeeper | Procurement, Legal, Value Analysis Committee | Vendor vetting, risk, contracting | Pre-approved BAA, SLAs, references |
A practical example we see all the time: marketing sends a "ROI one-pager" to a CMIO because they're labeled as a decision-maker, but the CMIO forwards it to IT with one line - "Do they integrate with Epic and support SSO?" If you don't already have the integration and security answers packaged up, the deal stalls before sales even gets a meeting.
Per this breakdown of healthcare buyer personas, the CIO cares about integration and total cost of ownership. The CMIO cares about evidence and clinical fit. The CFO cares about margin protection and payback period. If your content doesn't speak to each separately, you're donating deals to competitors who do.
Most teams create one whitepaper and blast it to the entire account. That's how you get ignored by four out of five decision-makers.
Compliance Basics (HIPAA, FTC, FDA)
HIPAA, FTC, and FDA aren't interchangeable acronyms you can wave at in a footer. They're three different rule sets, and mixing them up is how teams end up rewriting campaigns at the last minute.
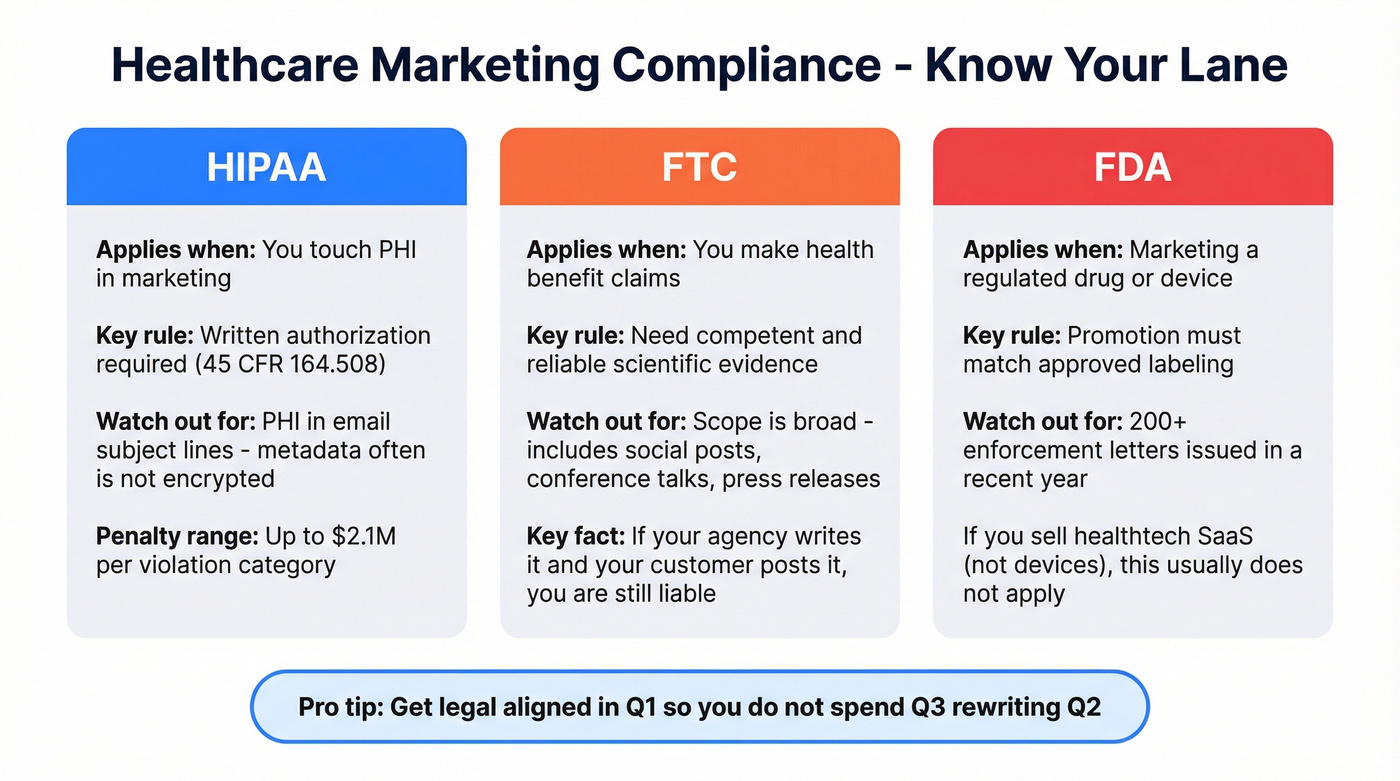
HIPAA: If you're using PHI in marketing, 45 CFR 164.508 requires written authorization, with narrow exceptions like face-to-face communications and promotional gifts of nominal value. Two rules keep you out of trouble more than any fancy policy doc: don't put PHI in email subject lines (metadata often isn't encrypted), and don't collect PHI through web forms unless the whole path is HIPAA-compliant end to end.
FTC: If you're making health benefit claims, you need "competent and reliable scientific evidence" before you publish. And the FTC's definition of advertising is broad: it includes trade show messaging, conference talks, press releases, influencer partnerships, and social posts, not just paid ads. If your agency writes the copy and your customer posts it, you're still on the hook.
FDA: If you're marketing a regulated drug or device, you're in FDA territory. FDA promotion enforcement has been active, with 200+ enforcement letters in a recent year. If you're marketing healthtech SaaS that doesn't touch regulated products, HIPAA and FTC are usually your primary constraints. Know which lane you're in, and get legal aligned early so you don't spend Q3 rewriting Q2.
Healthcare ABM only works when you can reach every stakeholder - the CMIO, the CIO, the CFO, and procurement. Prospeo gives you 30+ filters to target by job title, department, company size, and tech stack, then delivers 98% accurate emails so your carefully crafted role-based messaging actually lands.
Stop donating deals because your contact data bounced.
Why ABM Wins in Healthcare
When you're selling into accounts with 7-18+ month cycles and 15 stakeholders, broad demand gen turns into a slow bleed. ABM matches how these deals close: specific accounts, specific roles, specific objections, and a long sequence of "prove it" moments (build your target account lists first).
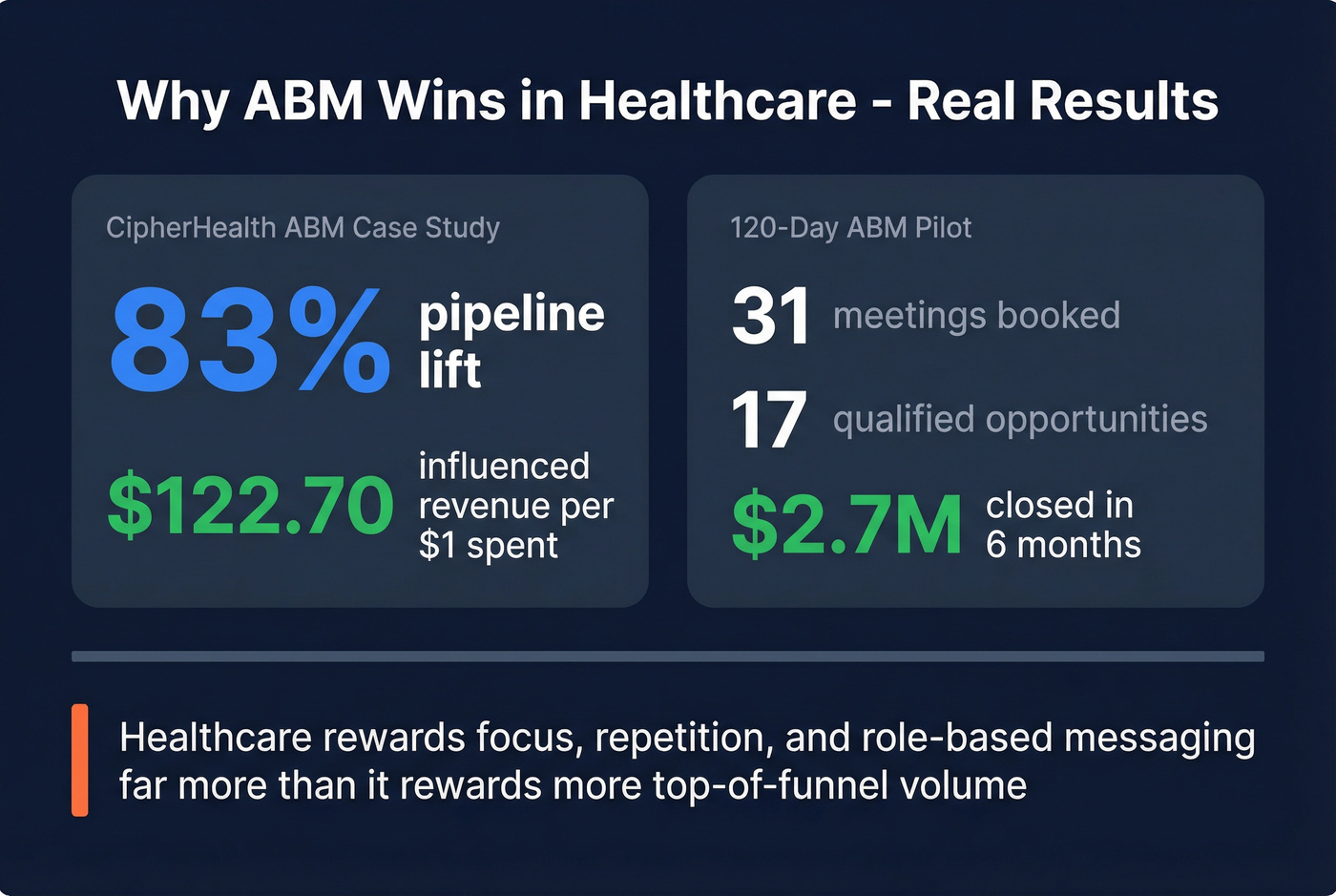
One ABM case study showed CipherHealth driving an 83% pipeline lift and $122.70 in influenced revenue per $1 spent. Another 120-day ABM pilot using intent data generated 31 meetings, 17 qualified opportunities, and $2.7M closed in six months. The point isn't that you'll copy those numbers. The point is that healthcare rewards focus, repetition, and role-based messaging far more than it rewards "more top-of-funnel."
Here's the thing: the tooling isn't the hard part. The execution gap is always the same. You've mapped accounts and personas, you've got a decent narrative, and then outreach falls apart because the contact data is stale or incomplete (fix the basics with an email deliverability guide).
We've watched teams burn through their entire addressable market in one campaign because they skipped verification. In healthcare, a bounced email isn't just a wasted touch. It's a domain reputation hit you can't afford, especially when your list is only a few hundred accounts and you need to keep sending for months (track it with email bounce rate benchmarks).
Hot take: if your ACV is closer to the low five figures, skip the six-figure ABM platform. A spreadsheet of 50 target accounts, Prospeo for verified contacts, and a sequencing tool will beat an overbuilt stack that nobody on your team actually uses (see account-based selling best practices for the sales-side motion).
The ABM assets that move deals
Let's break this down into a build order that works in the real world:
- Security + integration pack: SOC 2, architecture overview, SSO, audit logs, data flows, Epic/Cerner approach
- Clinical evidence pack: outcomes, study design, limitations, implementation notes
- Economic case: TCO model, staffing impact, avoided cost categories
- Procurement-ready docs: BAA template, SLA, insurance, subprocessor list
That's not "content marketing." That's deal acceleration, and it shortens the part of the cycle where everyone waits on someone else to answer basic risk questions (this is marketing enablement in practice).
Procurement Checklist (Before the Demo)
This is the checklist your prospect's security team often sends before they'll schedule a demo. If you don't have answers ready, the deal doesn't "pause." It quietly dies.
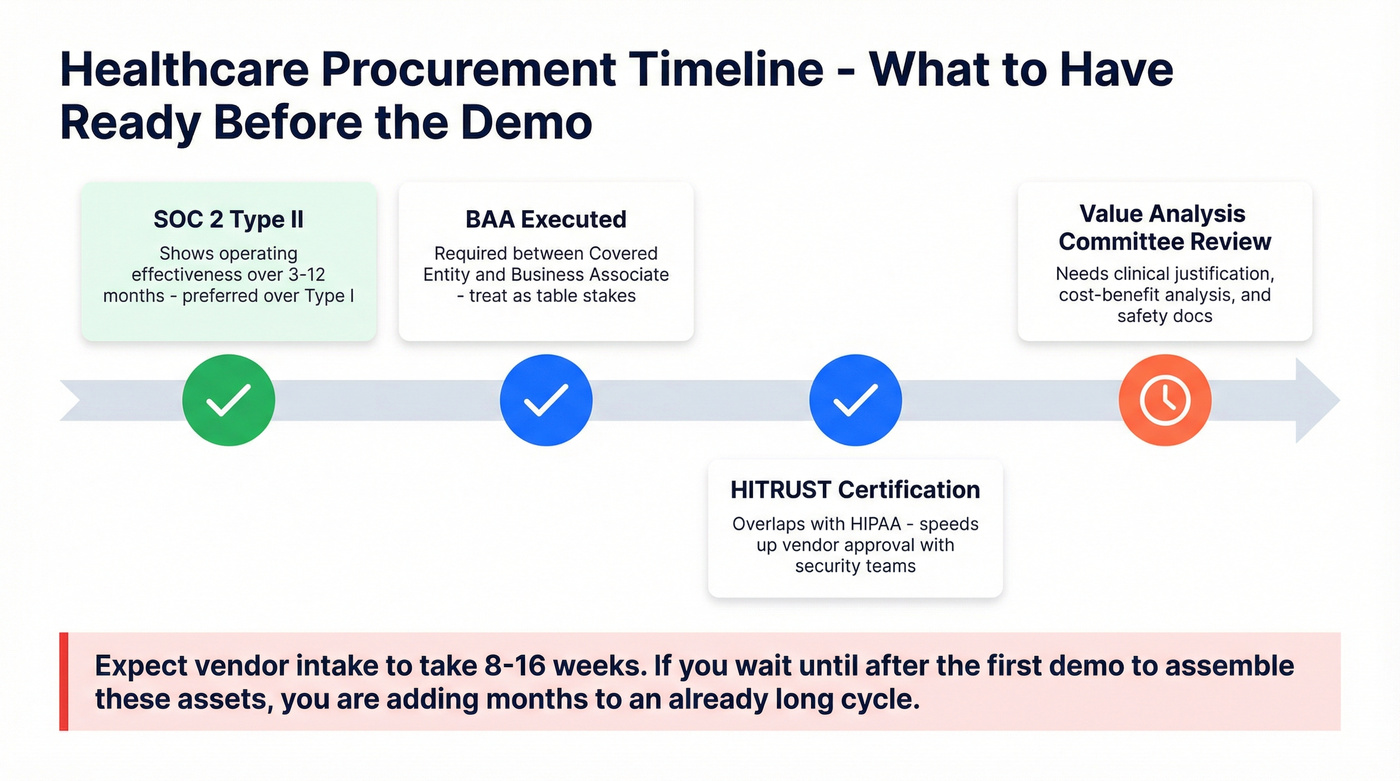
- SOC 2 Type II: preferred over Type I. Type II shows operating effectiveness over a period (often 3-12 months).
- BAA: required between any Covered Entity and Business Associate. Treat it as table stakes.
- HITRUST: it has significant overlap with HIPAA, and it often speeds up vendor approval because it gives security teams a familiar framework to score.
Expect vendor intake to take 8-16 weeks. Value Analysis Committee review adds its own timeline, and they want clinical justification, cost-benefit analysis, and safety documentation before anything moves forward. If you wait until "after the first demo" to assemble these assets, you're adding months to an already long cycle (use a product demo checklist to keep the process tight).
Mistakes That Burn Budget
Brochure thought leadership. Your "insights" piece is a product pitch with a different header. Clinical buyers see through it immediately. Lead with outcomes data, and be explicit about limitations so you don't sound like you're selling snake oil.
Writing for "providers" as one persona. We've seen teams send the same ROI whitepaper to a CIO and a CNO. The CIO wants integration architecture and security posture. The CNO wants workflow fit, staffing impact, and burnout reduction.
Sending outbound to unverified contacts. High bounce rates don't just waste a campaign. They tank your domain reputation and make every future send less likely to land (protect it with a plan to improve sender reputation).
One more that deserves a callout because it's so common: teams obsess over the perfect nurture stream, then they can't reliably reach the buying committee in the first place. That's backwards.
A practical contact-data standard
If you're doing outbound into health systems, set a hard internal bar:
- Bounce rate target: under 5% (under 3% is the goal)
- Role coverage: at least 5 stakeholders per account (economic, clinical, technical, champion, procurement)
- Refresh cadence: weekly, not quarterly (titles change constantly in hospitals)
Prospeo helps teams hit that bar with 300M+ professional profiles, 143M+ verified emails at 98% accuracy, and a 7-day refresh cycle. In practice, that means fewer dead inboxes, fewer "left the organization" replies, and a lot less time wasted rebuilding lists after every campaign (see data enrichment services if you’re stitching multiple sources).
Skip this if you're only running inbound and you never email prospects. If you're doing any outbound at all, though, data quality is deliverability.
When your addressable market is 50-200 health systems, every bounced email is a domain reputation hit you can't recover from. Prospeo's 7-day data refresh and 5-step verification keep your lists clean across months-long ABM sequences - at $0.01 per email, not $1.
Protect your domain and your pipeline with data that's verified weekly.
FAQ
What's a realistic CPL for B2B healthcare marketing?
A realistic CPL is about $377 on average, with healthtech SaaS around ~$130 and medical equipment closer to $609. Use 3-7% as a planning conversion range, then back into spend by channel and committee coverage. You're rarely converting one person; you're converting an account.
Which healthcare conferences matter most?
HIMSS, HLTH, ViVE, ATA Nexus, and AHIP are the safest "big five," and each maps to a different buyer set across providers, payers, digital health, and health IT. Plan for 2-3 events per year max, and pick based on your ICP and integration story, not the biggest booth or loudest keynotes.
How do I build a verified healthcare contact list?
Start by mapping five roles per account (economic, clinical, technical, champion, procurement). Pull contacts by title and department, then verify before you send. Prospeo's real-time verification and 98% verified email accuracy make it a strong fit for healthcare outbound, especially when you need to cover multiple stakeholders per account without burning your domain.
Summary
B2B healthcare marketing works when you stop "marketing to providers" and start engineering the deal: committee-specific messaging, compliance-first claims, ABM execution, and procurement-ready assets. Pair that with verified contact data so your outreach lands, and you'll build pipeline without lighting budget on fire.